전공의 2년차 말인 2019년 11월에 작성하여 전공의 3년차인 2020년 3월에 출판된 원저 논문입니다.
수련 때 미용과 함께 가장 많이 한 수술은 피부암이었습니다. 피부과에서 피부외과를 보지 않았기 때문에 펀치조직검사를 해서 수술을 해야하는 경우 성형외과로 의뢰하였습니다. 이 중 보웬병이 참 많았는데, 보웬병(Bowen's disasea)는 한마디로 "Intraepidermal squamous cell carcinoma" 즉, 피부에서 표피내에 국한 된 편평상피세포암입니다. 조금 더 진행하면 편평상피세포암이 된다는 말이죠. 그래서 SCC의 전암병변이라고도 합니다.
Moh's microsurgery라고 피부과에서 많이 하기도 하지만, 아직 성형외과에서 편평상피세포암에 준하여 광범위절제술과 동결절편을 하여 실시간으로 수술방에서 정상피부병변에 침투된 암세포가 없는지 확인하고, 이로인해 생긴 결손을 국소 피판술이나 피부이식술 등으로 덮어주는 경우가 많습니다.
얼굴에 크게 구멍이 뚫리는 경우가 많은데 (크게는 지름 4~5cm정도) 이를 주변 조직을 잘 이용하여 재건해주면 감쪽같이 티가 안나는 경우가 많습니다. 이 병변에 대해서는 피부과에서 쓴 논문들이 많아 우리 성형외과에서 접근한 방식대로 역학과 그 수술방법 등에 대하여 분석을 해보기 위해 연구한 논문입니다.
Data Collection & Data Analysis
데이터를 일단 모아야겠죠?
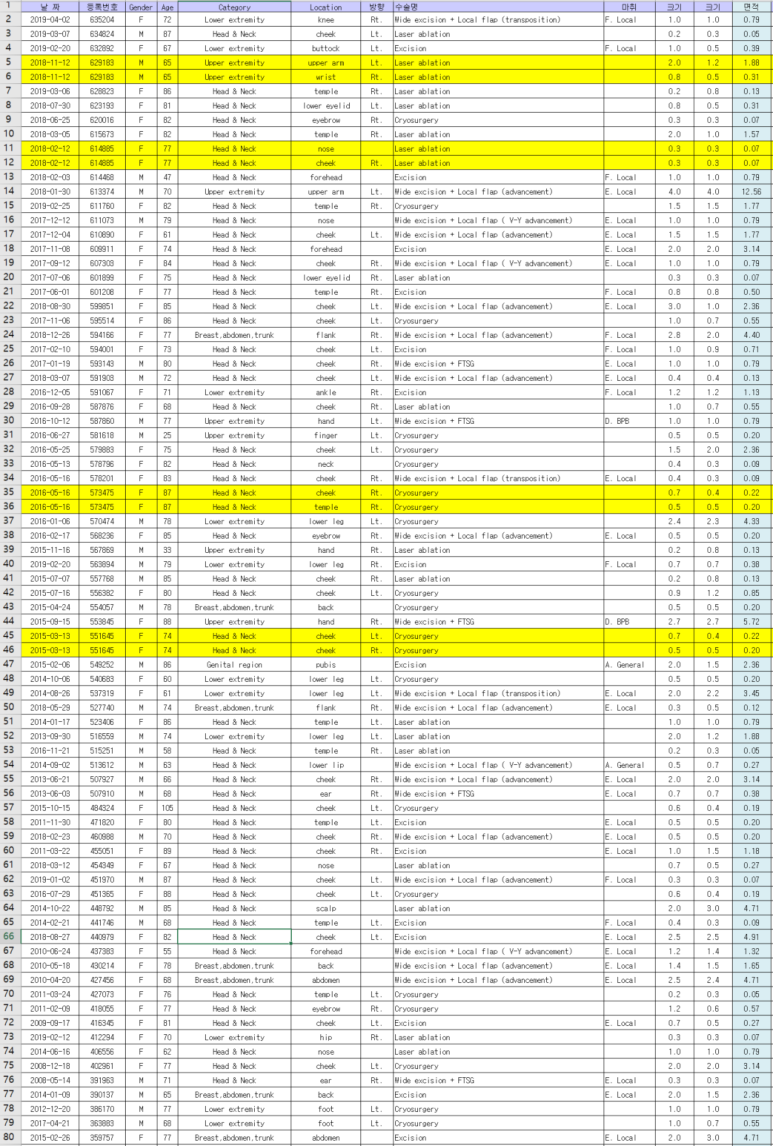
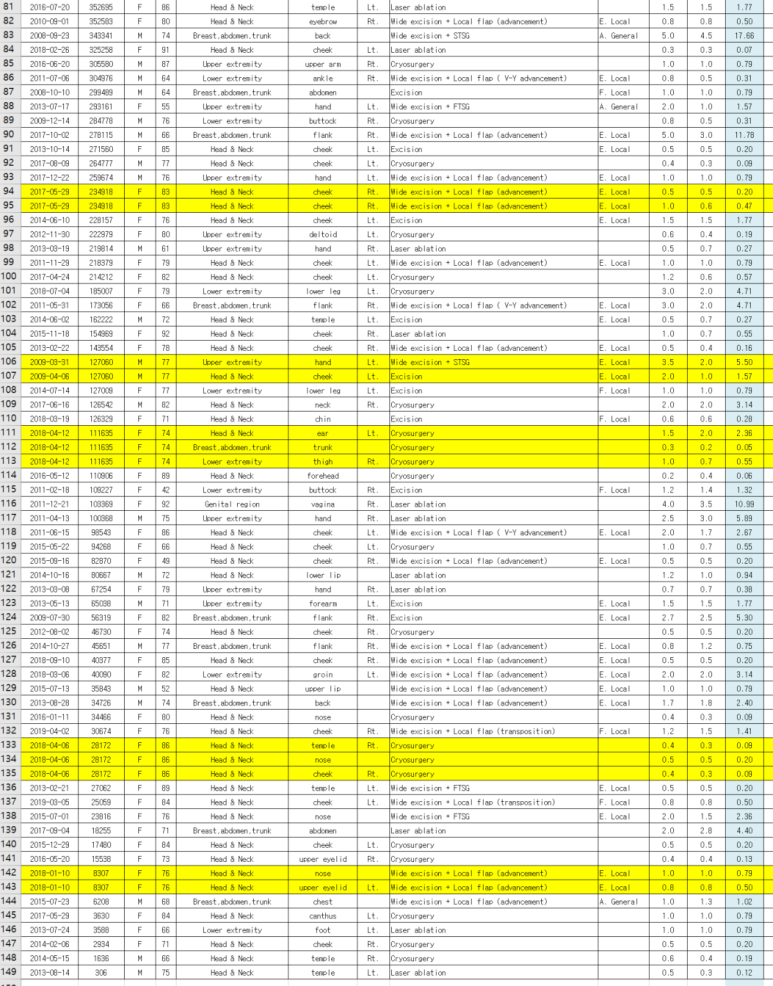
우선 이렇게 raw data를 모은 후에,
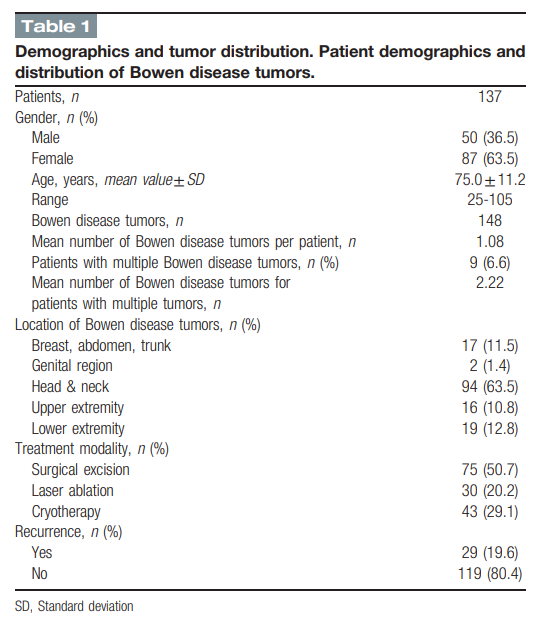
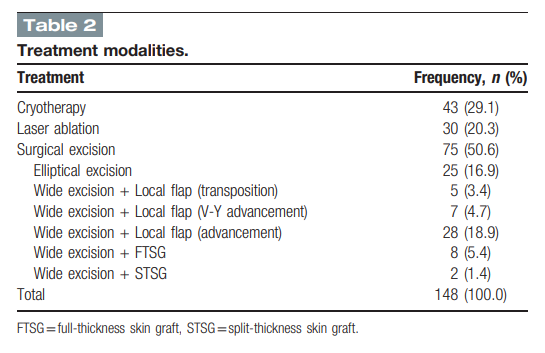
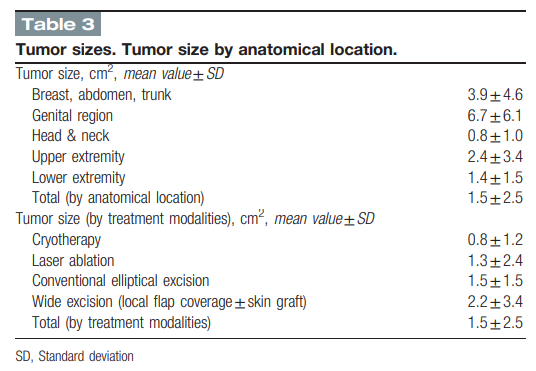
이렇게 아래와 같이 간단한 기술통계를 냅니다.
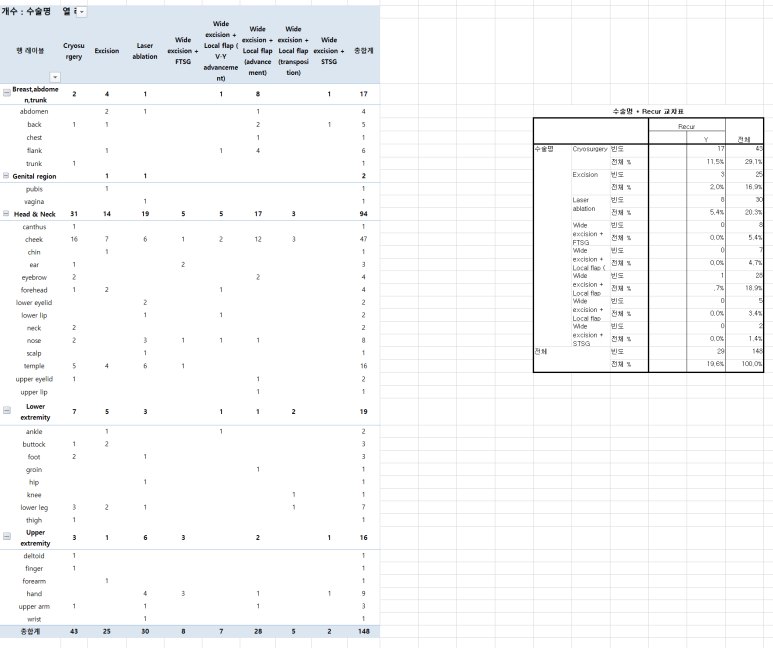
의학통계분석에는 기술통계와 분석통계가 있는데 간단한 기술통계 (빈도, 최빈값, 중앙값, 최소 최대값 등)는 Excel에서 바로 가능하기도하고 spss에서도 쉽게 구할 수 있습니다.
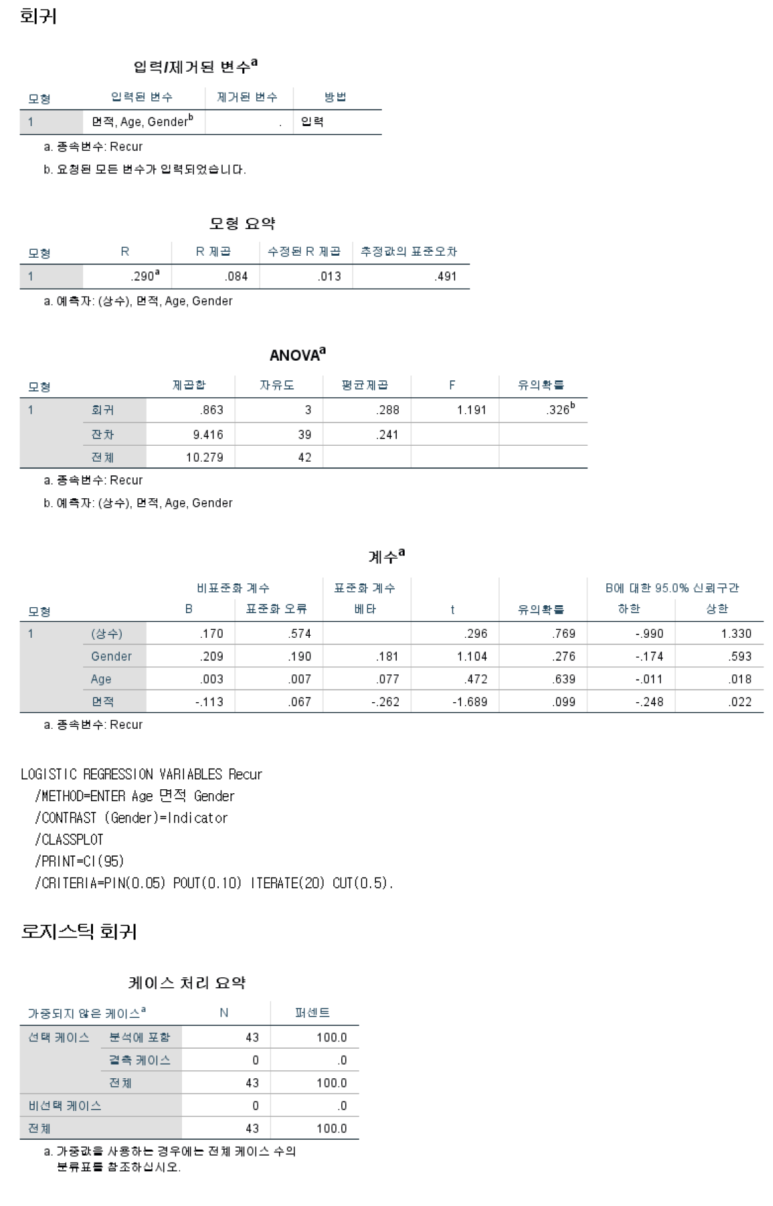
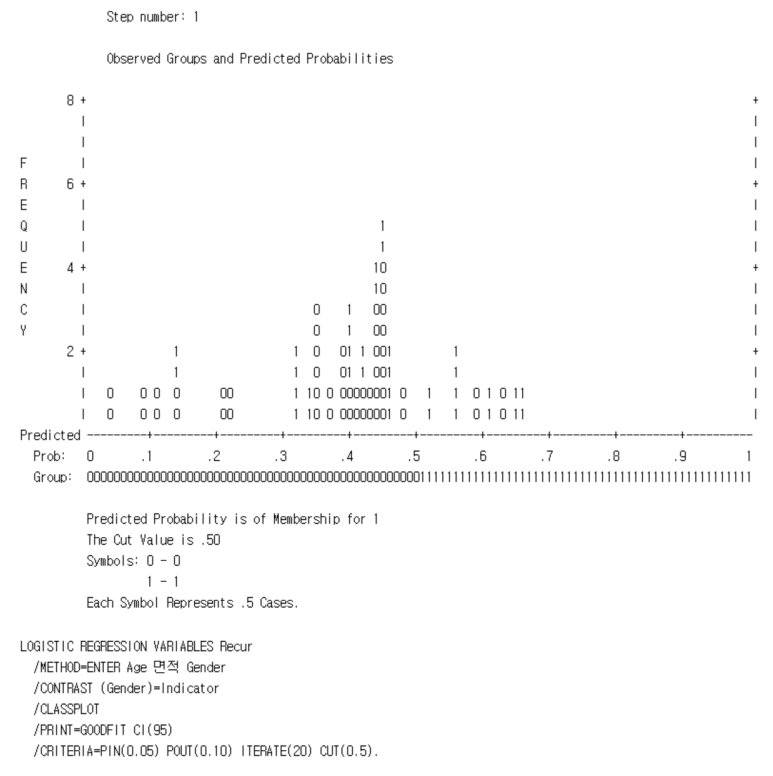
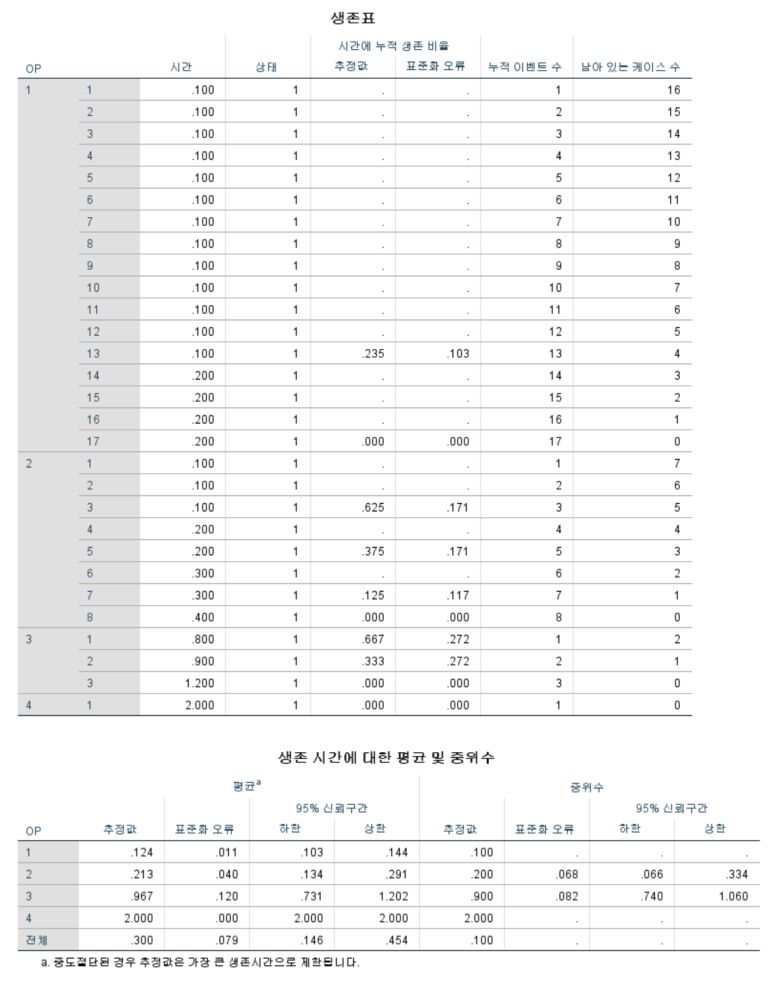
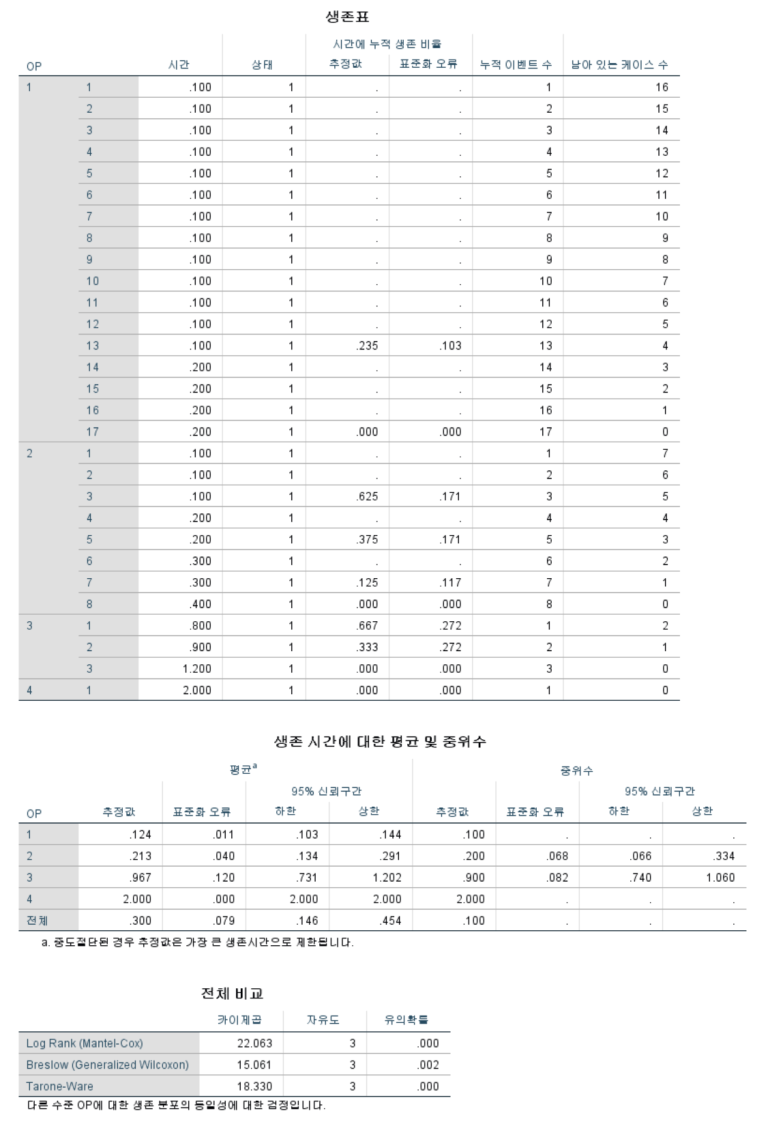
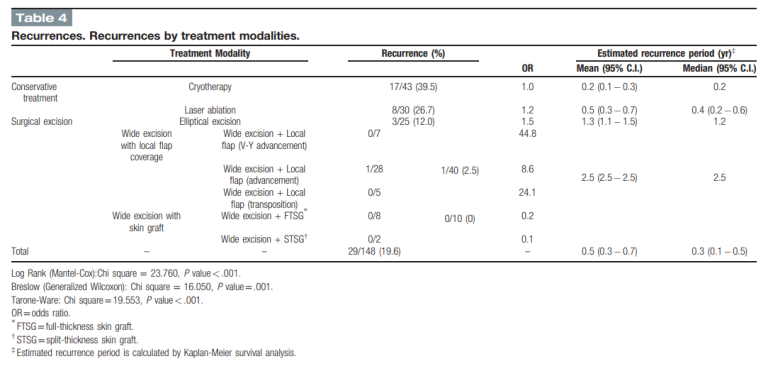
SPSS로 분석통계도 돌렸고, 통계 결과상 나온 결론을 바탕으로 논문의 결론과 discussion부분을 완성하였구요, 특히 생존분석(제 연구에서는 재발율) 관련된 부분은 카플란 마이어 분석으로 재발율을 예측했습니다.
피부암은 완전히 절제하여 재발하지 않게 하는 게 가장 환자를 위한 치료이죠.
피부암을 초기에 피부과에서 많이 보기 때문에 대부분의 피부암에서 Moh's microsurgery가 TOC 이긴하지만,
저는 성형외과에서 차라리 Wide excision 후 frozen section 을 하여 완전히 제거 했는지 확인한 뒤,
flap이나 skin graft로 wound 를 resurfacing하고 흉터관리를 하여 완전히 치료하는 게
더 나은 방법이라고 생각합니다.
그래서 성형외과에서 하는 술기들도 비교하여 여러 방법들 간에 재발율 차이도 비교해보았습니다.
우선 아래 사진들을 피부암 절제 후 사용하는 여러 수술 방법들과 결과입니다.
Figures
단순 일차봉합으로 간단하게 끝내고 흉터관리 하는 방법들이 있고요
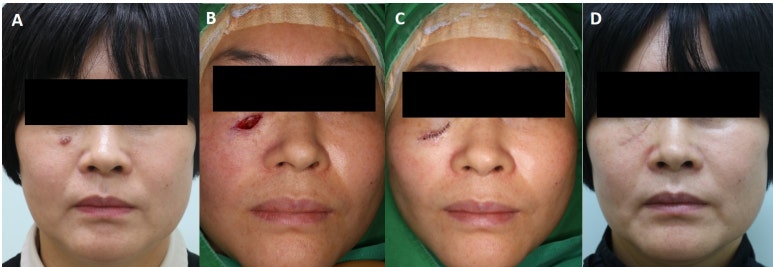
Figure 1: Conventional elliptical excision on the right lid-cheek. A, A 0.5 × 0.9 cm2 sized rapidly growing Bowen disease tumor on a right lid-cheek. B−C, After conventional elliptical excision, the defect was closed using a primary simple interrupted suture. D, A curvilinear scar remained on the right lid-cheek at 3 weeks postoperatively.
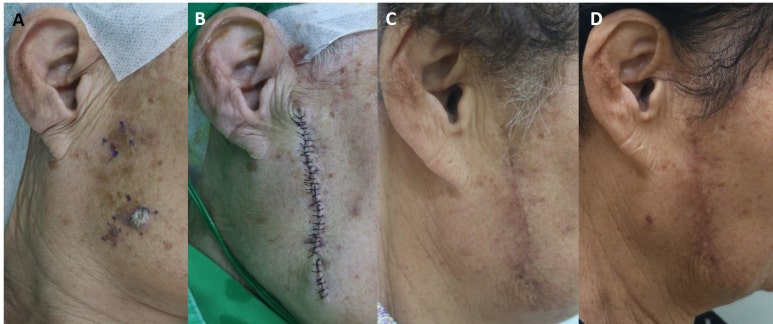
Figure 2: Wide excisions with a local flap (advancement). A, A 75-year-old woman visited our outpatient department with three Bowen disease tumors (all were histopathologically confirmed) on her right cheek (preoperative clinical photo). B, Wide excision with local flap coverage was performed. After undermining, both flaps were advanced and sutured. C, Clinical photograph of the hypertrophic phase taken at 1 month postoperatively. D, No complications, such as contour deformation, margin irregularity, or recurrence, were evident at 6 months postoperatively, though mild melanocyte migration was observed.
일차봉합으로 끝내기 힘든 경우는 각종 국소피판술로 덮을 수도 있습니다.
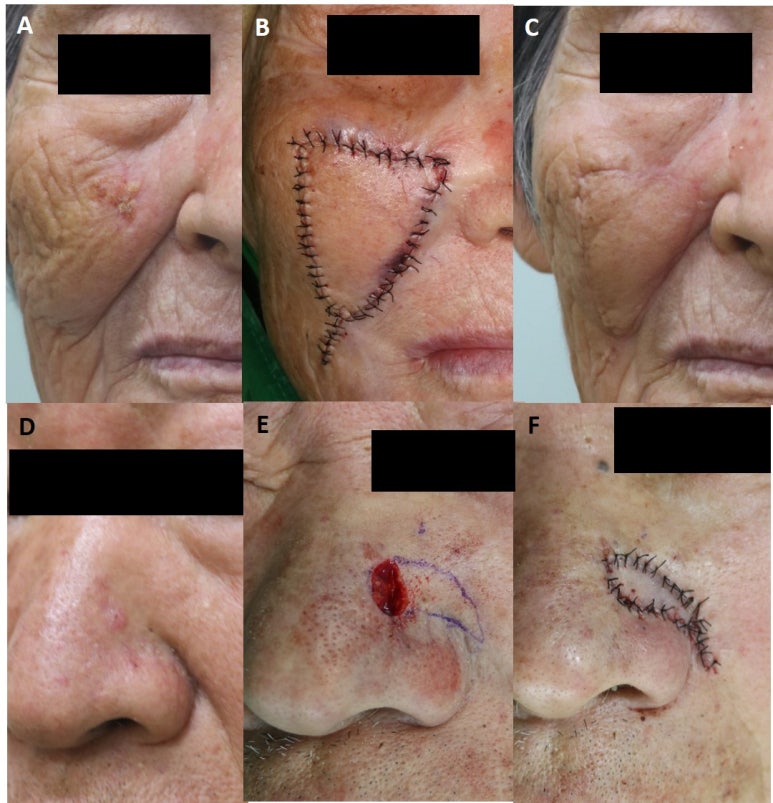
Figure 3: Wide excisions with local flap (V-Y advancement). A-C, A 1.2 × 1.5 cm2 sized Bowen disease tumor on a right lid-cheek. After wide excision, the defect was resurfaced using a V-Y advancement ipsilateral cheek flap. D-F, The defect was closed using a V-Y advancement flap based on underlying nasalis.
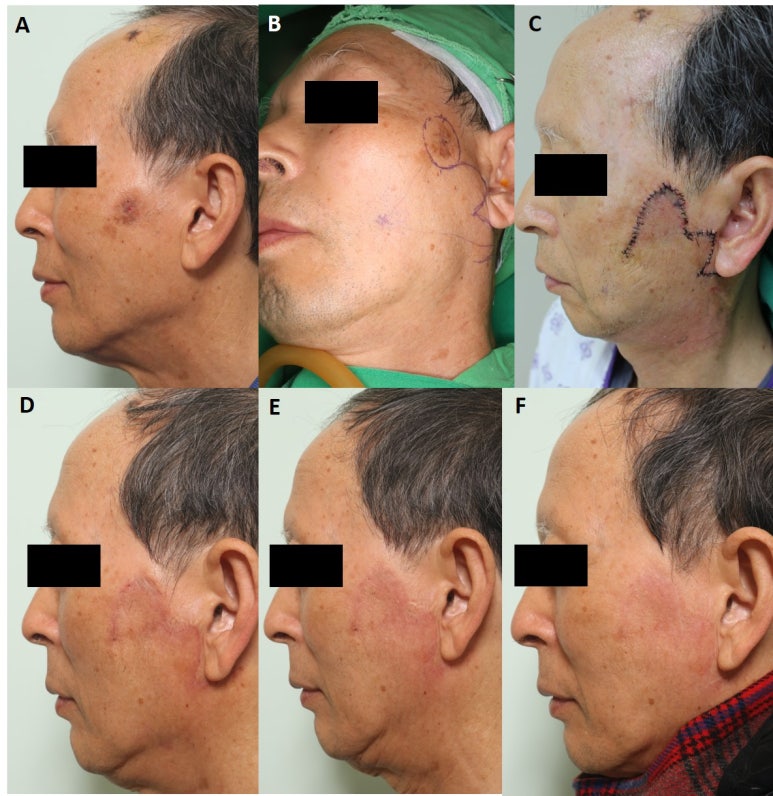
Figure 4: Wide excisions with a local flap (transposition). A, A 71-year-old man visited our outpatient department with a histopathologically confirmed Bowen disease tumor on his left cheek. B−C, After wide excision of the tumor, the defect was resurfaced with a geometric bilobed flap (a type of transposition flap). Adequate undermining, proper flap thickness, and counter-clockwise flap rotation resulted in no skin tension or venous congestion. D−F, Clinical photos taken at 1, 2, and 6 months postoperatively. The wound matured with time and the scar faded.
아래와 같이 피부이식술로 깨끗하게 낫게 할 수도 있어요.
피부이식술이 나은 부위는 따로 정해져 있습니다!
아무곳에나 하면 안돼요. 코 바로 옆에 내측 눈꺼풀 옆쪽은 전층피부이식으로도 주변과 이질성 없이 깨끗하게 나을 수 있는 부위죠.
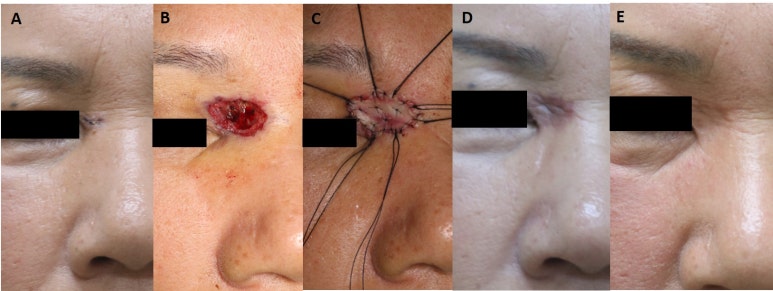
Figure 5: Bowen disease. Wide excision with a full-thickness skin graft (FTSG). A, Photograph showing a Bowen disease tumor on right medial canthal area. B, A small subcutaneous defect remained after wide excision of the lesion. C, The defect was resurfaced with full-thickness postauricular skin graft. D, One-month postoperative photo. E, At 1 year postoperatively, the recipient site scar had matured substantially. FTSG = Full-thickness skin graft.
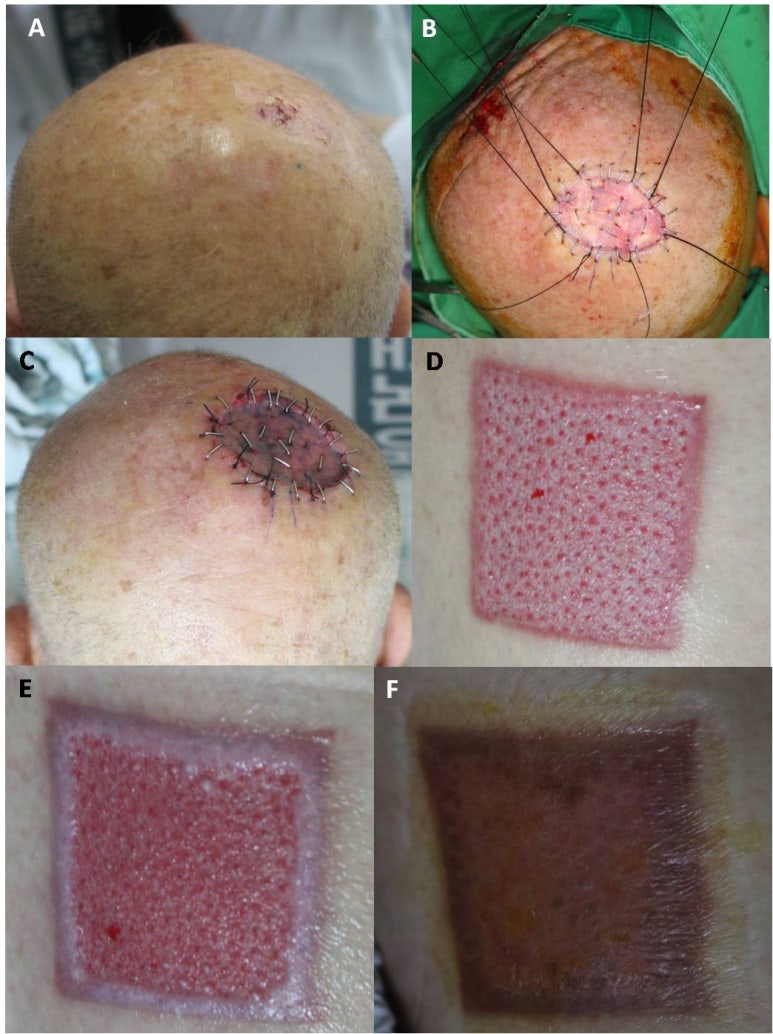
Figure 6: Wide excisions with a split-thickness skin graft (STSG). A, A 78-year-old man visited our outpatient department with a histopathologically confirmed ∼2.0 × 2.0 cm2 sized Bowen disease tumor on his occiput. B−C, After wide excision of the tumor, the defect was resurfaced with a split-thickness (10/1000 in) skin graft harvested from his left thigh using an air dermatome. D−F, Clinical photos of left thigh donor site at 1, 3, and 5 weeks postoperatively. The donor site defect was resurfaced by secondary intention using a simple foam dressing. Epithelialization initiated at the defect margin and the wound was completely epithelialized at about 5 weeks postoperatively. STSG = Split-thickness skin graft.
Tables
간단간단한 기술통계들은 spss에 나온 표를 그대로 excel로 옮겨 조금 다듬고 MS word스타일로 바꿔 투고를 하면 아래와같은 이쁜 표로 알아서 바꿔줍니다
분석통계에서 조금 어려운 생존분석인데요.
통계학적으로는 생존분석이지만, 우리가 하는 연구에서는 피부암의 재발이지요.
'사망' 을 '피부암의 재발' 로 생각하고 발생율을 알아보는 거지요.
피부암을 완전히 절제하였음에도 아주 조금씩 예기치 않은 재발이 일어나는 이유를 모식도로 그린 그림입니다.
주변에 그림 잘 그리는 형 도움을 받아 직접 그리고 작성한 illustration입니다.
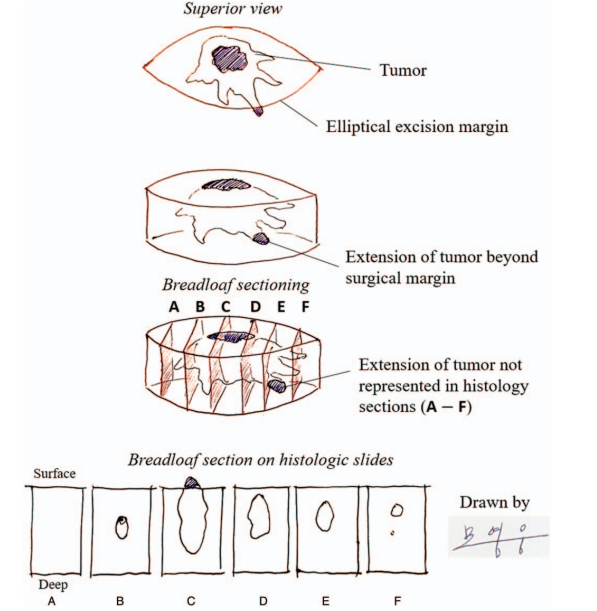
Figure 7: Limitation of the breadloaf biopsy sampling method when examining the margins of conventional elliptical excisions.[16] In this example, excisional tip breadloaf sections A and F were clear of tumor, but sections B, C, D, and E demonstrated tumor. Furthermore, extension to the peripheral margin was not detected in any section, and thus, the excision was technically clear on margins. However, this margin assessment was inaccurate. Extension of tumor to the surgical margin between sections D and E was missed
이렇게 투고를 해서....
보통 외과영역에서 역학분석에 대한 논문을 투고하는 medicine에 투고를 했고 몇 개월간의 review를 거쳐, 한 번의 minor revision 후 accept되고 publish됐습니다.
아래는 전문입니다
생존분석 통계는 처음으로 공부해서 돌려본건데, 보통 내과나 일반외과영역에서 암의 5년생존율 구할 때 쓰는 카플란 마이어 통계분석입니다. 우리 성형외과에서는 피부암을 수술하니 피부암의 재발율 이 곧 사망율이 되겠네요.
원리를 이해하면 참 괜찮은 분석 같습니다.
통계학자들은 어떻게 이런 방법들을 생각해서 어떻게 프로그램에 적용시켜놓았을까요?
자연과학의 위대함이란... ㅎㅎ
데이터가 다 준비되어있으면 통계분석, 논문 작성, 영문 교정, 통계 교정, 투고까지...
총 2~3주 정도 걸릴 것 같습니다.
데이터가 많으면 굳이 수술방법 소개가 아니더라도 역학분석도 참 의미있는 연구 같아요.
그럼 또 다음 논문 포스팅에서 뵙겠습니다
방문해주셔서 감사합니다!