Zygoma reduction surgery is a procedure that many people considering reducing the contours of the midface are curious about and interested in.
My philosophy regarding zygoma reduction surgery, based on more than 10 years of experience and long-term follow-up, is as follows.
First, zygoma reduction surgery should be different from simple zygoma reduction.
Second, after zygoma reduction surgery, the appearance should continue to improve over time.
Third, the area that expresses the three-dimensionality of the face (the malar highlight) should be preserved in zygoma reduction surgery.
Fourth, cheek sagging should not occur after zygoma reduction surgery.
Fifth, after zygoma reduction surgery, the condition of the bone should be such that even from immediately after surgery, light pressure or chewing hard food does not affect the position of the bone.
In other words, when reducing the contour of the zygoma that forms the outline of the midface, one should make the utmost effort to create a beautiful zygoma shape.
If one is focused only on reducing the volume of the zygoma while damaging its three-dimensionality,
then when postoperative swelling remains in the early stage, it may not be noticeable, but as time passes after surgery, the face may end up with an awkward, flat, or deflated-balloon-like contour.
As suggested by the classical saying too much is as bad as too little, the process of surgery produces irreversible results, so overcorrection can become the biggest problem.
In order to preserve the three-dimensionality of the midface after zygoma reduction surgery, I think it is appropriate to maintain a certain amount of volume in the zygomatic body just below the outer corner of the eye. Here, too, if overcorrection is performed, even though one may feel satisfied during the period when swelling still remains to some extent and feel that the contour of the zygoma has been reduced, the face can become more planar as time passes.
The zygoma reduction surgery I perform involves selecting appropriate methods depending on the case, and among patients who have not previously undergone surgery elsewhere, the proportions are as follows:
-
Partial osteotomy of the body and complete posterior osteotomy of the zygomatic arch, followed by fixation of the posterior zygomatic arch area 70%
-
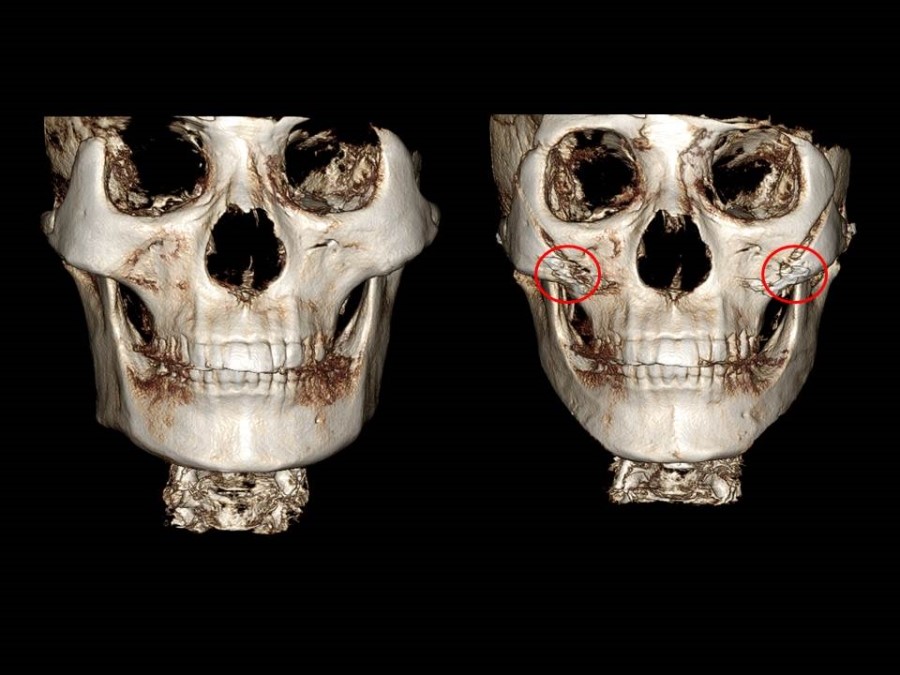
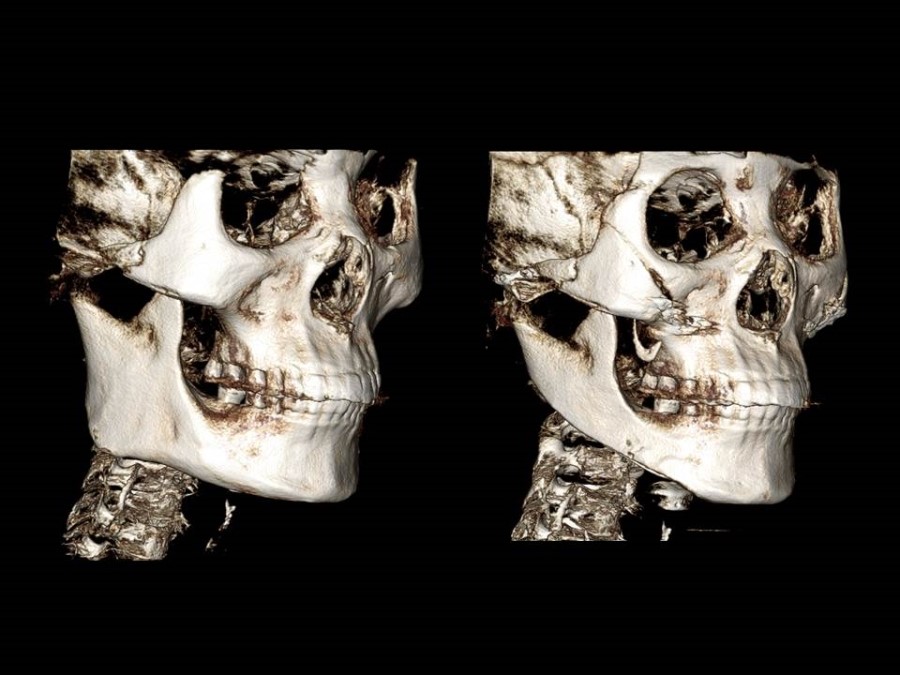
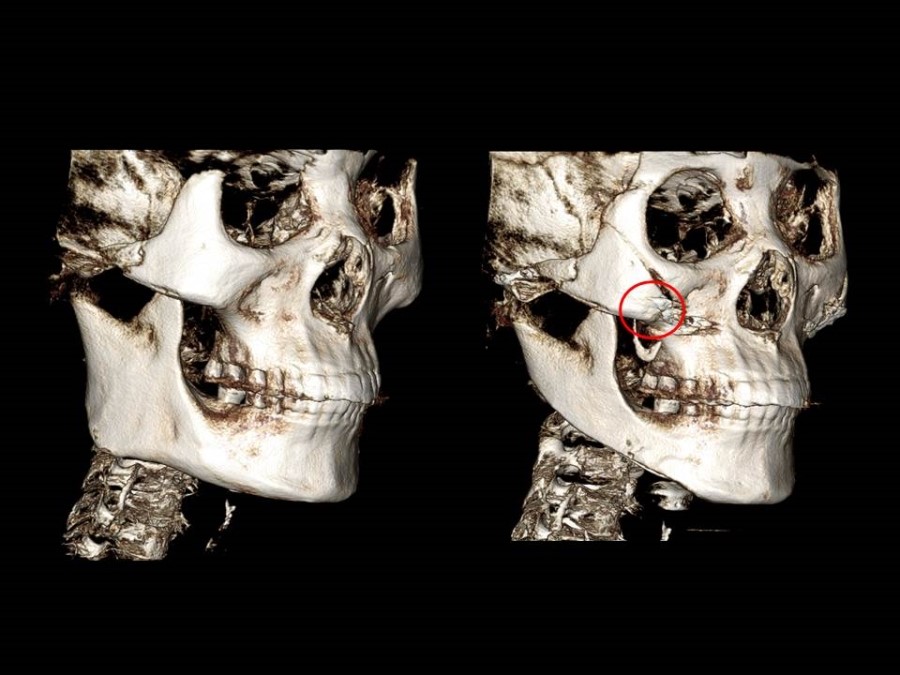
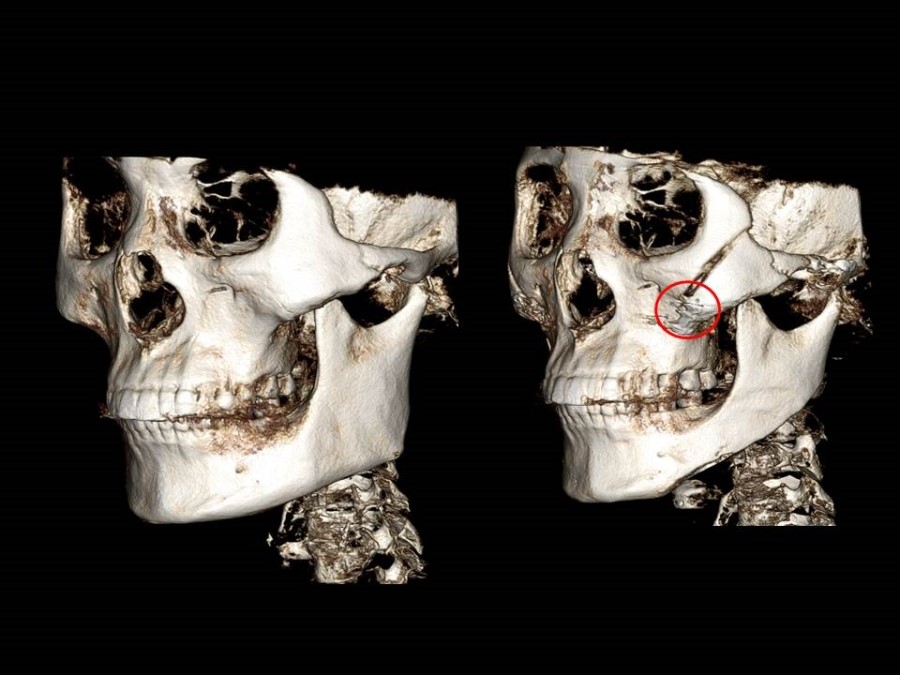
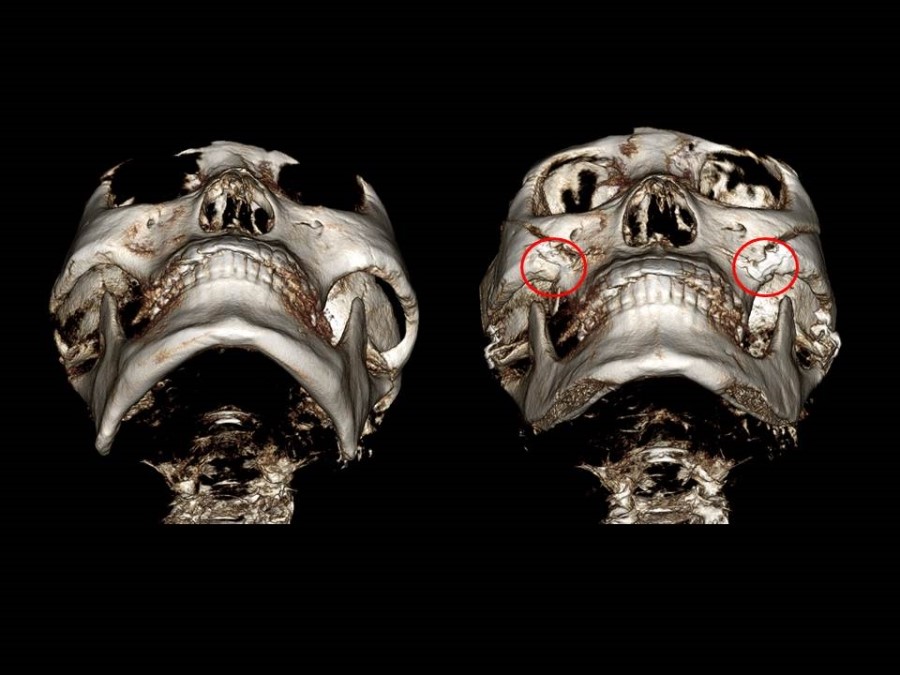
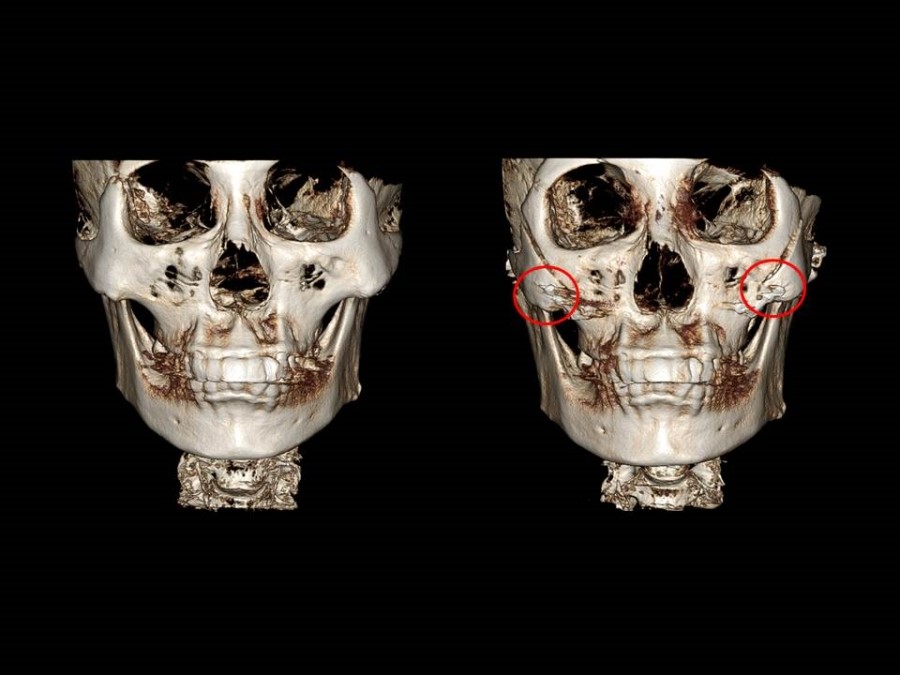
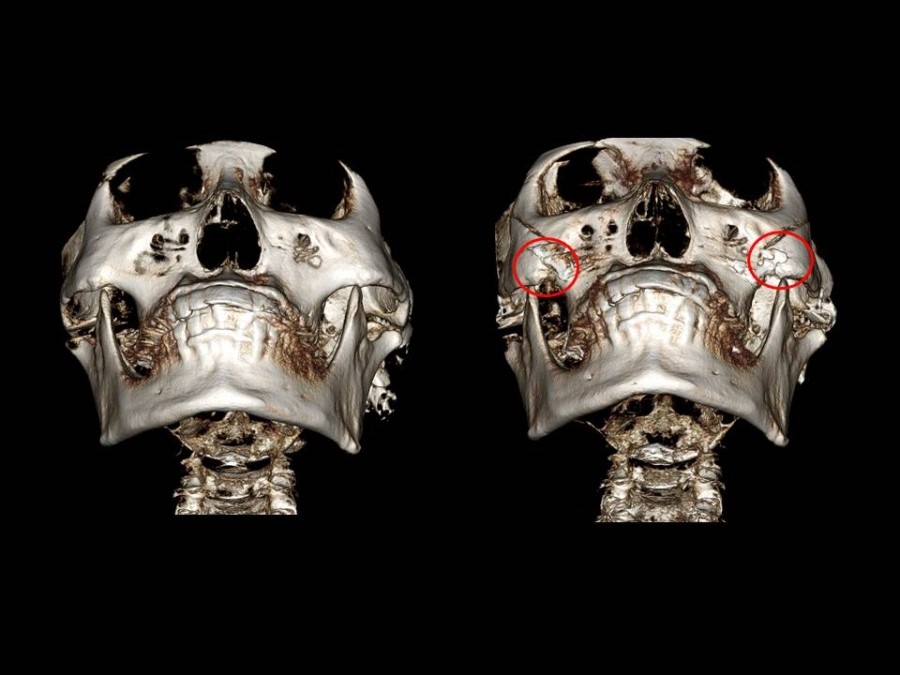
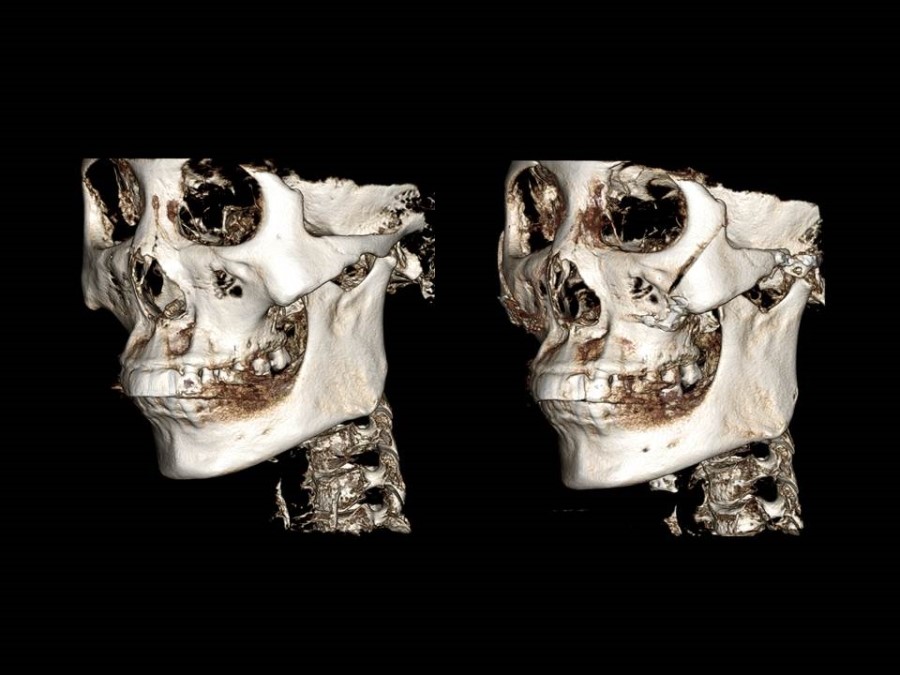
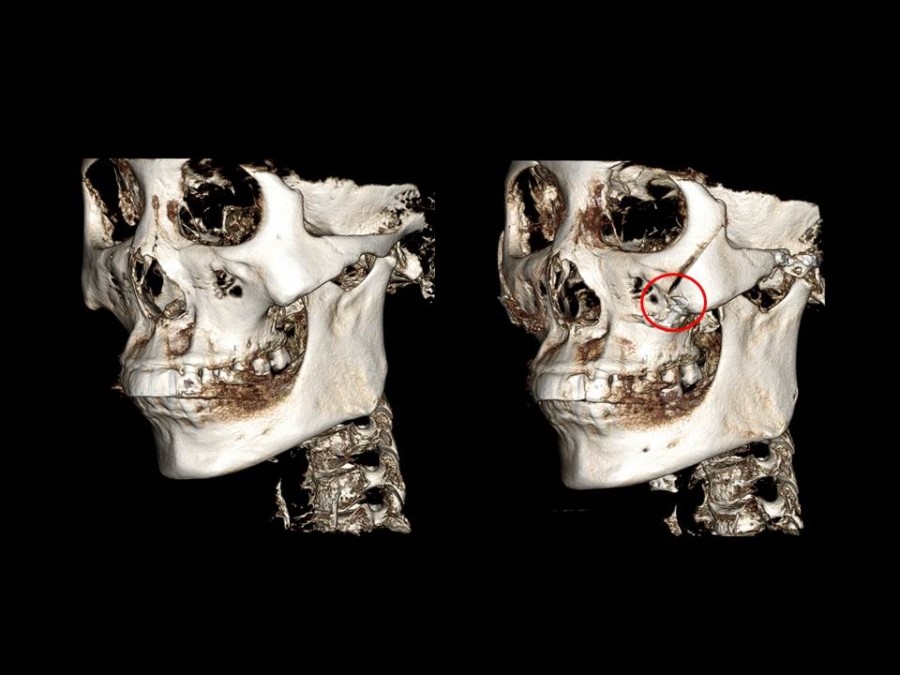
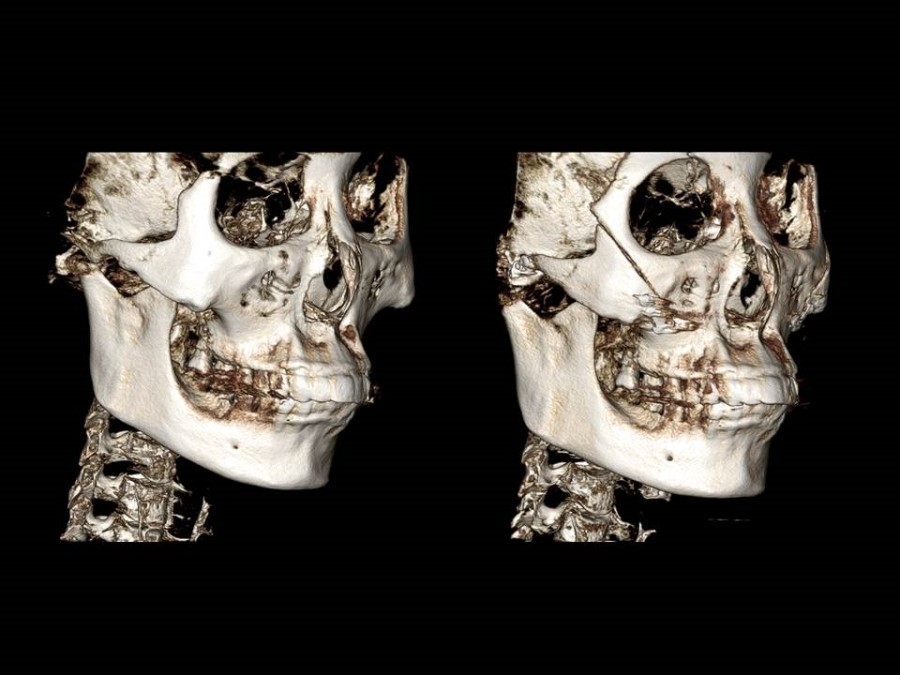
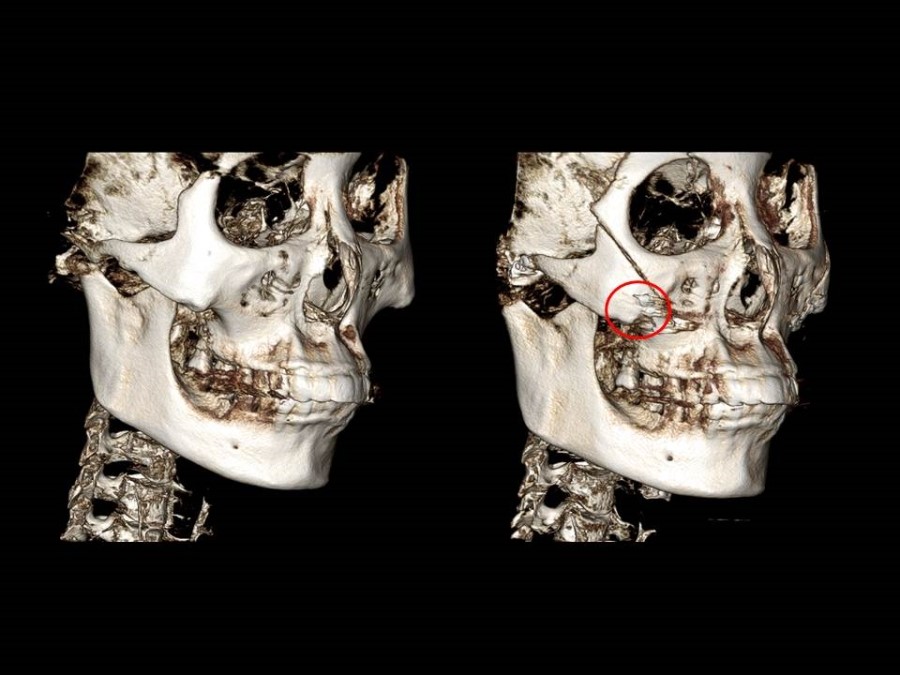
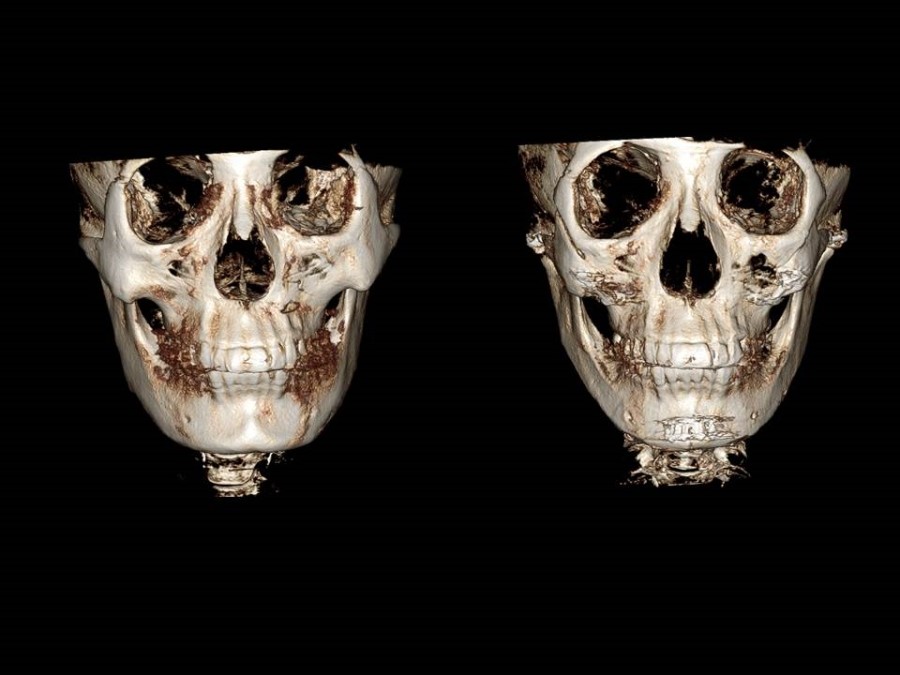
Complete osteotomy of the body and posterior zygomatic arch area, followed by fixation at two points, the body and the arch 20%
-
Bone shaving to reduce only the zygomatic body 10%
When selecting the above surgical methods, the most important consideration is the shape of the zygoma before surgery, and the personality and expectations of the patient also have an influence.
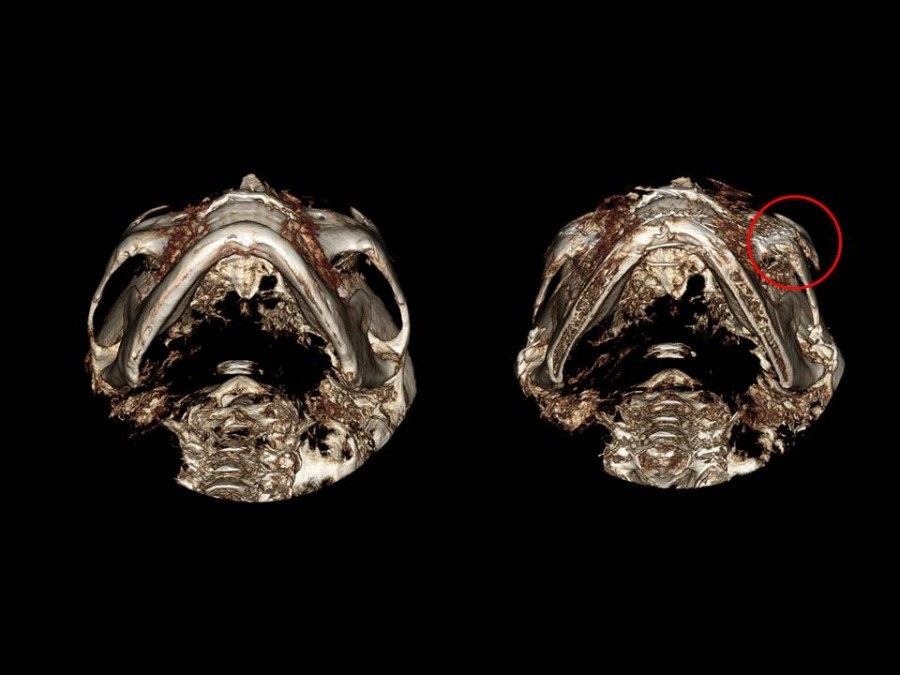
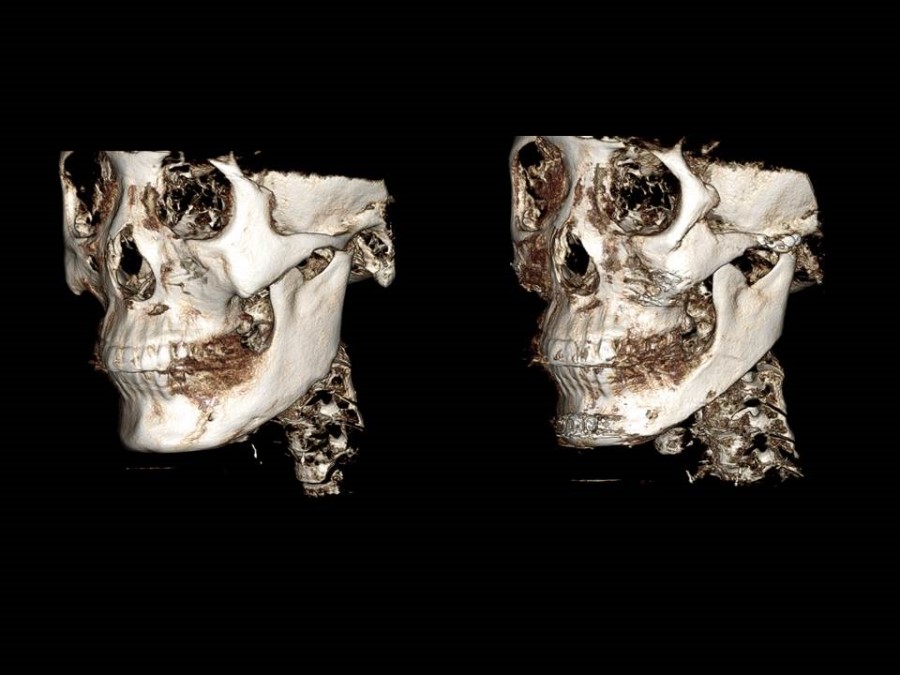
Below are the pre- and postoperative 3D CT images of patients who underwent complete osteotomy of the body and zygomatic arch with fixation at two points.