When considering surgery to reduce the contour of the zygoma, which defines the contour of the central part of the face, the most important point is which area to reduce and in what direction to reduce it.
In zygoma reduction surgery, the part I consider most important is that, while preserving facial three-dimensionality, the width of the face should be narrowed so that, after the zygoma contour changes, a younger and more lively appearance can be expected.
Sometimes, during consultations, there are people who say they would like the zygoma reduced so much that its shape disappears altogether.
As the saying goes, too much of a good thing can be bad,
it seems we busy and impatient people sometimes forget the very important truth that something excessive is worse than something lacking.
In any case, facial shapes vary from person to person, and the areas that are developed differ as well.
Therefore, when performing surgery to reduce the contour of the zygoma, I believe the most important thing is to choose a method that appropriately reduces the developed areas of the zygoma.
As I emphasized in my post about V-line square jaw surgery, my view is that there is a problem when facial shapes are all different but the surgical method is uniform.
First, medically speaking, the zygoma is called the malar complex or zygomatic complex.
As the term complex suggests,
the zygoma is composed of the malar body (zygomatic body) and the malar arch (zygomatic arch).
Looking at the faces of various people who want the zygoma contour reduced,
there may be cases where the body is developed, and there may also be cases where the arch is developed.
Therefore, I believe the most ideal approach is to choose the appropriate surgical method depending on which area needs to be reduced more.
I divide cases of zygoma prominence into two broad categories when selecting a surgical method.
-
When the body of the zygoma is developed (in the figure below, the area marked with a blue circle is the body of the zygoma.)
-
When the zygomatic arch is widened (in the figure below, the area marked with a red circle is the zygomatic arch.)
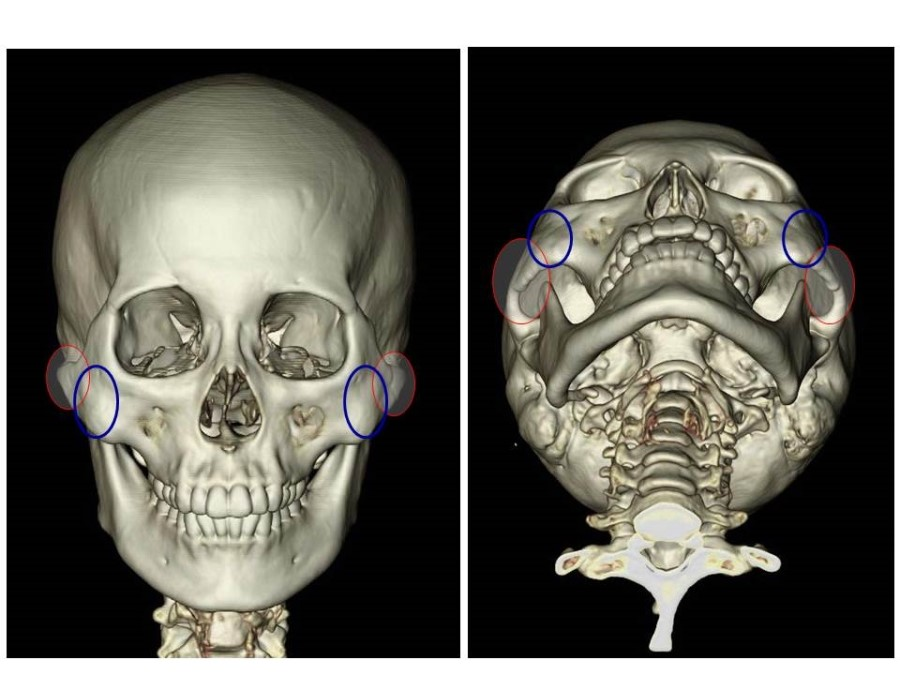
Looking at the different zygoma shapes from an upward-facing angle, they are as follows.
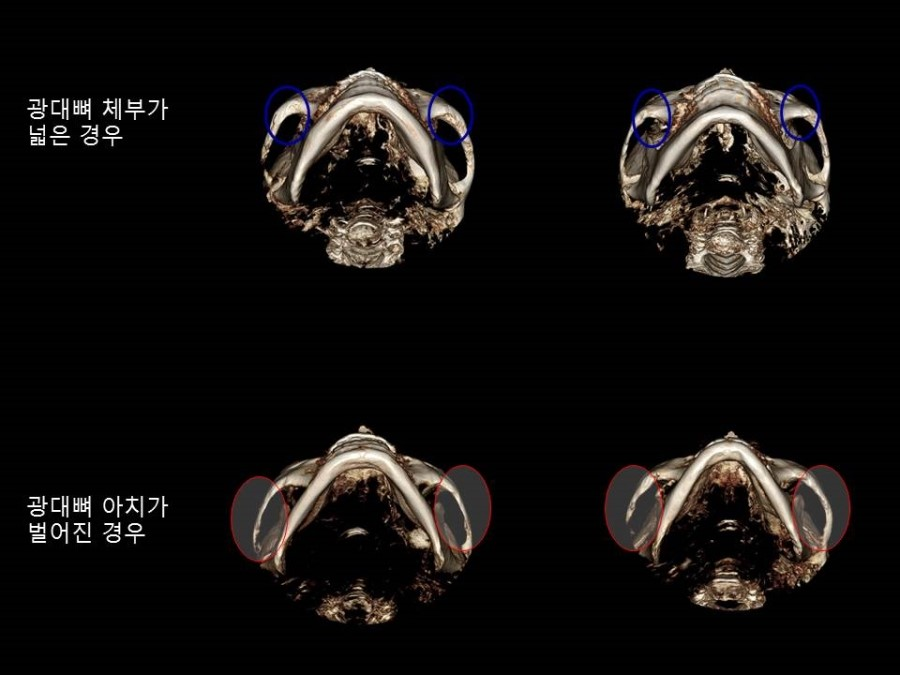
From the CT images above,
in cases where the body of the zygoma is developed, as in the top two cases,
I think it is appropriate to perform surgery by completely osteotomizing and fixing both the zygoma body and the posterior part of the zygomatic arch.
In cases like the bottom two, where the zygoma body is not prominent but the zygomatic arch is widely spread backward,
I think it is appropriate to perform a partial osteotomy of the zygoma body, then completely osteotomize the posterior part of the zygomatic arch and bring the widened arch inward.
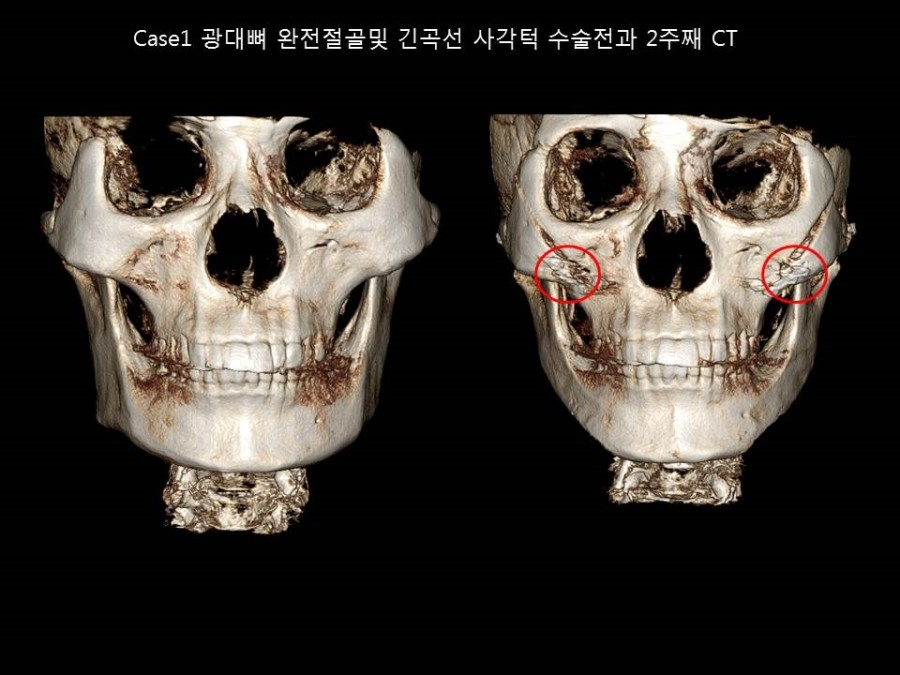
Below is a case in which the zygoma body was developed, and both the body and the posterior part of the zygomatic arch were completely osteotomized and fixed.

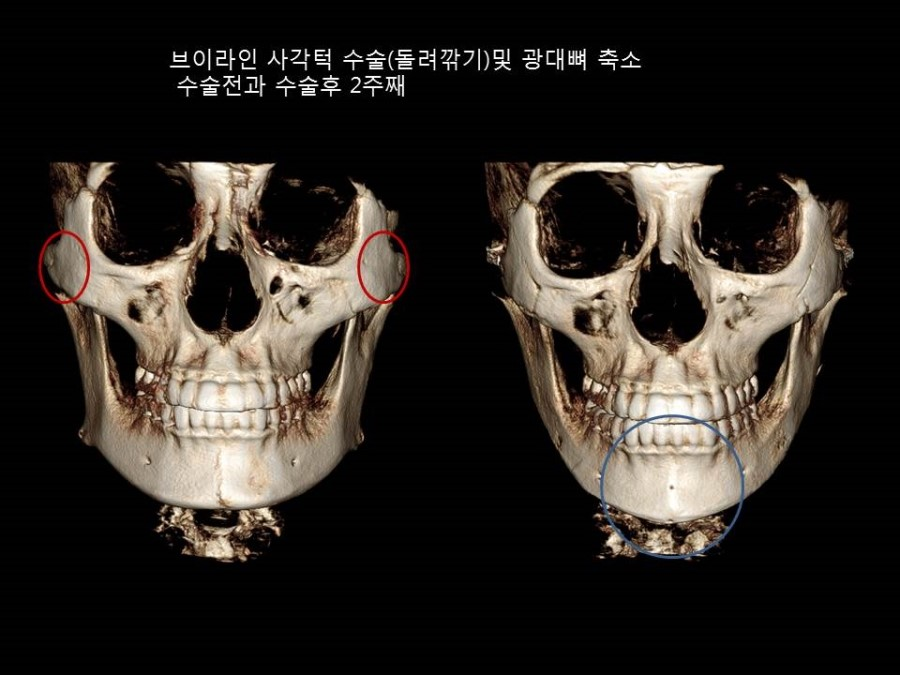
Next is a case in which the zygomatic arch was widened, and the appropriate surgical method was to perform a partial osteotomy of the body and a complete osteotomy of the posterior arch.


In conclusion, depending on the shape of the face before surgery, I believe it is appropriate to choose the proper surgical method according to which area is being targeted for reduction.