Several decades ago, a person who made a living by reading physiognomy visited me to have the contours of the zygoma corrected. At a glance, the zygoma was clearly prominent, and the impression was not soft. In physiognomy, prominent zygomatic bones suggest a harsh fate, so for that person, it was necessary to work on the zygoma both to improve their fortune and for their profession as a physiognomist.
There is no need to go as far as physiognomy. There are cases where a prominent zygoma causes a poor first impression. When people greet each other or talk, they always tend to look into the other person's eyes. In terms of facial contours, the zygoma forms the contour around the eyes. When the zygoma contour is prominent, the face not only looks wide and flat, but the impression can also seem strong and stubborn.
In modern times, when “appearance” and “first impressions” have become even more important, the number of people considering zygoma contour surgery continues to increase. Most East Asians who consider zygoma contour surgery tend to hope that a face that looks wide and rugged from the front will change into a narrower, softer, and more three-dimensional face.
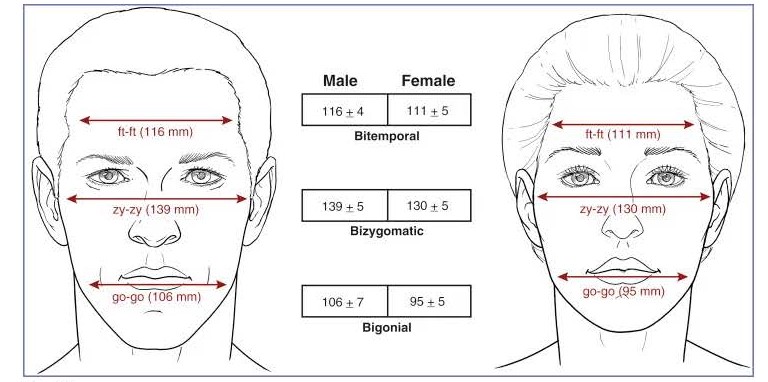
When the face is divided into three sections, the most important area responsible for the contour of the middle third, the midface, is the zygoma, which plays a central role in determining facial width. If you measure the horizontal width of the facial bones from the front and examine the statistics, the distance at the temple area is 111 mm, the width at the zygoma is 130 mm, and the distance at the angular part of the lower jaw is 95 mm, meaning the zygoma area is statistically the widest part of the face (Fig. 1)
If the surgery is performed accurately and effectively, one can expect a width reduction of about 7 to 10 mm on one side of the face. However, with zygoma reduction surgery, the degree of change that can be expected may vary depending on the condition and structure of the facial bones before surgery. Among the contour surgery cases I have operated on, there were four pairs of twin sisters.
In two of those pairs, identical twin sisters underwent zygoma reduction surgery elsewhere and came to me for a second surgery. Strangely, although they were twins, the places where they had their first surgeries were different. Because they had each undergone the first surgery elsewhere using different methods, the condition and status of the zygoma when I performed the surgery showed many differences despite them being twins, and as a result, the degree of postoperative change also differed.
This is how zygoma surgery is performed.
First, if you are concerned because the zygoma is prominent, it is necessary to accurately identify which area is prominent. The medical term for the zygoma is the “zygomaticomaxillary complex.” It may sound somewhat difficult, but “zygoma” means the cheekbone, and “complex” implies that it is composed of the body and the arch.
The contour of the middle part of the face formed by the zygoma (zygomaticomaxillary complex) can be broadly divided into the front zygoma and the side zygoma. The front zygoma is the area that appears to project forward below the eyes, and the side zygoma is the area that appears to project laterally among the facial contour lines connecting the temple to the lower cheek when viewed from the front.
These days, the area that transitions from the front zygoma to the side zygoma is sometimes called the “45-degree zygoma,” and the farthest back portion of the side zygoma is called the “posterior zygoma.” Generally speaking, the front zygoma is formed by the zygomatic body, which corresponds to the body of the zygoma, while the side zygoma is formed by the zygomatic arch.
Most people considering zygoma contour surgery want a face that is smaller and softer instead of a wide, flat one, while also wanting a more three-dimensional contour. However, if the direction of surgery is wrong, it is not uncommon to see cases where the flat appearance does not improve even after zygoma surgery, and the loss of dimension makes the face look even flatter.
Moreover, zygoma reduction surgery is one of the operations that can lead to unfortunate results if an inexperienced surgeon does not precisely check the osteotomy position and condition of the bone and does not properly fix the moved bone in its new position.
So how is zygoma surgery performed?
Surgery to trim a large, prominent zygoma into a smaller and softer shape is usually performed through the inside of the mouth, with a small incision made in the sideburn area of the skin. This is done to make the externally visible surgical scar less noticeable.
In particular, the direction of zygoma surgery that I consider most important is not to cut away part of the bone and reduce it, but to move the bone inward while preserving bone continuity completely.
Fortunately, because there is sufficient space on the inner side of the zygomatic arch, that space should be used to move the prominent zygoma area so that a smaller, softer facial shape can be achieved while preserving three-dimensionality.
There are these pitfalls in zygoma surgery performed by non-specialists.
However, it is essential to remember that there are many pitfalls for those considering zygoma contour surgery. If you are concerned about a prominent front zygoma or 45-degree zygoma, a relatively simple method of reducing the protruding zygomatic body through an incision only inside the mouth may provide effective improvement. But if you hope to improve a contour line that appears somewhat prominent from the front as it runs from the temple to the cheek, or if you expect the overall facial width to be effectively reduced, it is necessary to consider side zygoma reduction, including the posterior zygoma. To effectively and safely change the contour of the side zygoma, it is necessary to move the zygomatic arch inward and fix it in the correct position.
Surgery to refine the shape of the facial bones located deep beneath the skin requires the experience and anatomical expertise of a highly skilled surgeon. Yet recently, there have occasionally been advertisements that try to replace medical reality with sweet-sounding claims, such as saying that this highly difficult surgery can be completed simply within just over ten minutes or that no special fixation materials are used. If surgery were performed according to these advertisements, what would happen? The most common complications would be nonunion and cheek sagging.
-
Nonunion refers to a case in which the bone at the artificially cut site during zygoma surgery does not properly join and instead separates, leaving a gap. Common causes of nonunion include insufficient fixation of the cut bone during zygoma surgery or excessive removal of part of the zygoma. If nonunion occurs, the bone does not remain stable, may droop downward, or the facial contour may partially collapse, making the face look uneven.
-
Cheek sagging is a phenomenon in which the nasolabial folds become deeper after zygoma surgery and the skin in the cheek area appears to sag downward. The most common cause of cheek sagging can be a surgical method that cuts away part of the zygomatic body responsible for the front zygoma contour.
The retaining ligaments surrounding the facial bones play an important role in preventing the soft tissue around the face from separating from the bone. If this area is cut away during surgery, postoperative cheek sagging may inevitably occur.
In addition, if the zygomatic body area responsible for the front zygoma contour is cut away, the three-dimensional quality of the face may disappear and it may become more flat. As a result, the face may lose its lively appearance compared with before surgery and instead end up looking older, which can be an unfortunate outcome.
Surgeries to consider together
The most important point for those considering zygoma contour surgery is the overall harmony of the facial contours.
In face shapes where the lower face looks angular and prominent, reducing only the zygoma can make the overall facial contour somewhat more rectangular, creating a risk that the face will look heavier and more gloomy.
To avoid ending up with a peanut-shaped face after zygoma contour surgery, it is necessary to consider combining the procedure with surgery that reduces the muscles and fat pads that create volume in the temples, as well as surgery that removes deep cheek fat in the area below the zygoma.
If both the side zygoma and the temple area are generally wide, it is important to consider reducing the muscles and fat pads that create volume in the temples at the same time as zygoma reduction surgery.
If you are middle-aged and your skin elasticity has decreased somewhat, it is advisable to consider a facelift together with zygoma contour surgery.
Conversely, if you are considering a facelift to lift a sagging face, prominent side zygomas may become even more noticeable because of the facelift, so it may be wise to consider zygoma contour surgery as well.
Precautions after surgery
After zygoma surgery, once the major swelling has subsided and the bone condition has stabilized, a CT scan must be performed to check whether the bone after surgery is maintaining a stable position. Occasionally, people who had zygoma contour surgery in the past come in for consultation feeling desperate after belatedly realizing that the bone at the surgical site has separated, even though they had not known the state of their bone. If the bone is not fixed in a stable state after zygoma surgery, the gap may widen over time and part of the bone may be resorbed, so it is necessary to check as soon as possible and take appropriate measures. And after confirming on CT that the bone is stable, it is important to start mouth-opening exercises as early as possible to loosen the temporomandibular joint area.