Based on the case of a patient who underwent zygoma reduction surgery with me two weeks ago, I would like to explain some points that many people may be curious about.
In the clinic, some of the explanations I give during consultations and the guidance I provide about postoperative progress and care for patients who have actually undergone surgery may differ from the commonly spread general notions, so I think there may be cases where people feel anxious and have questions.
A person who had previously undergone bimaxillary surgery at another medical institution 10 years ago came to see me for a consultation in March of last year (2020), wanting to improve the prominent zygomatic contour of the area connecting the temples to the cheeks.
The metal fixation hardware in the maxilla and mandible had not been removed after the bimaxillary surgery, but the zygomatic area had never been operated on.
Considering the overall contour, the lower face appeared somewhat more prominent on the right than on the left, while the contour of the midface was slightly more prominent on the left than on the right.


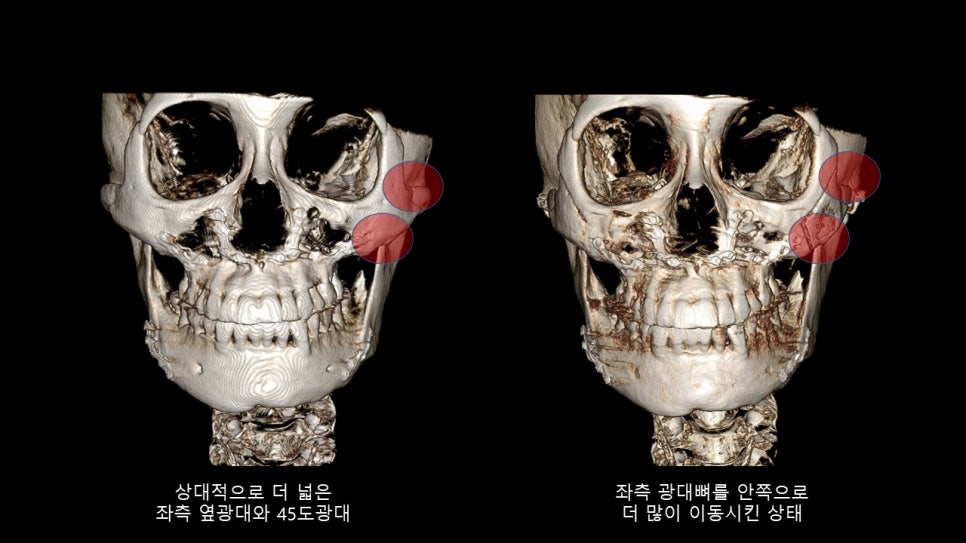
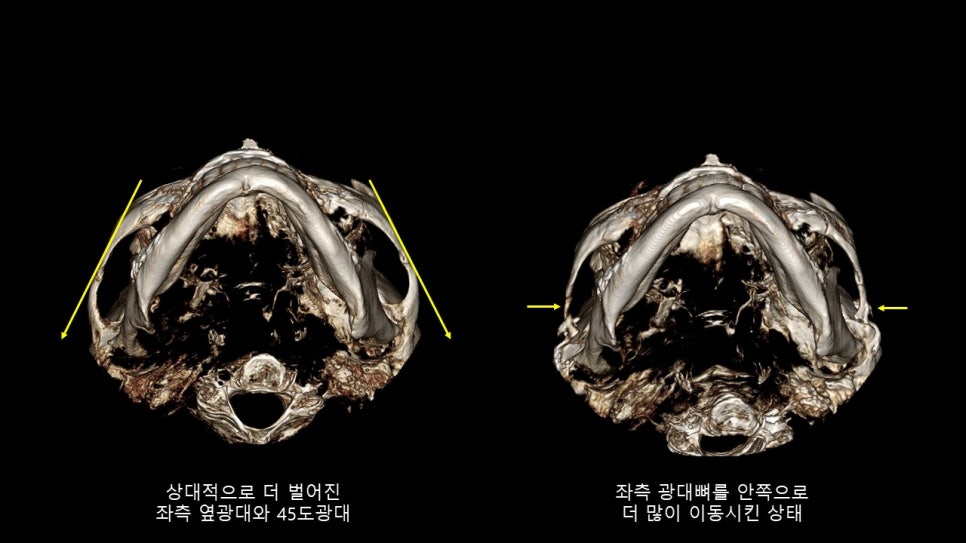
3DCT seen from the front and from the base during the consultation last March
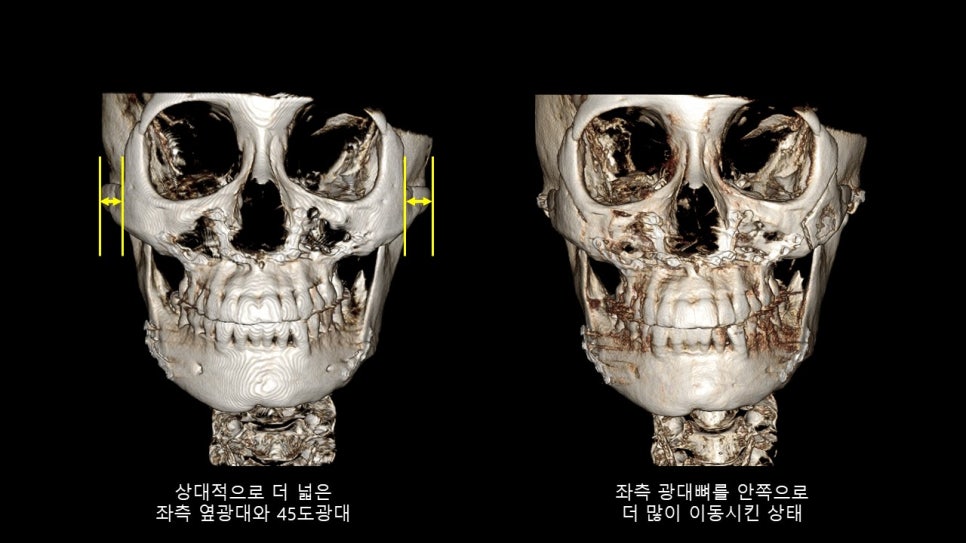
- For improving the contour of the midface
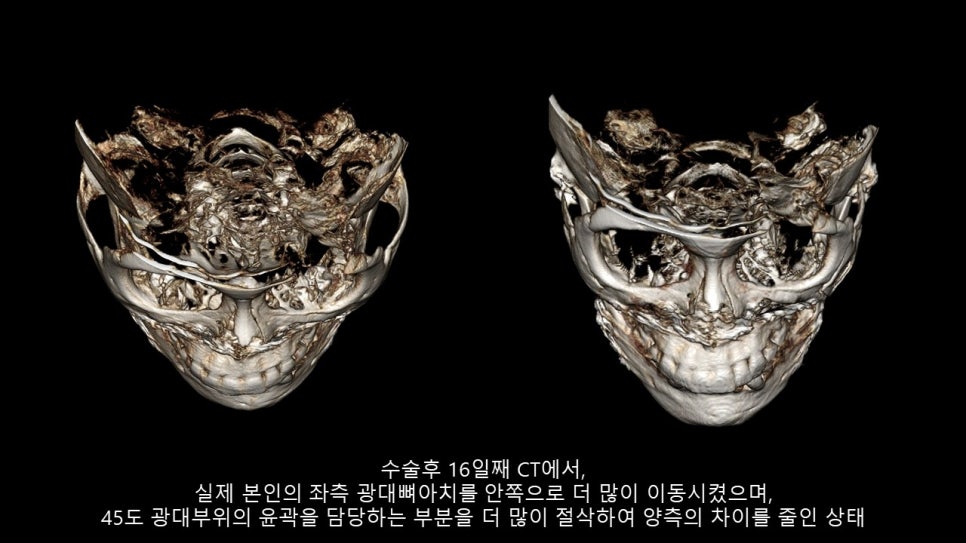
Through zygoma reduction surgery, I thought it would be better to soften and smooth the pronounced contour line of the area connecting the temples to the cheeks when viewed from the front, and I judged that it would be appropriate to reduce the left lateral zygoma, which appeared somewhat wider than the right, relatively more.
- For improving the contour of the lower face
I thought that removing the metal fixation hardware attached to the body of the mandible, which appeared more prominent on the right, and reducing the body of the mandible as much as possible would be helpful.
After the first consultation, the patient returned for another consultation about 1 year and 8 months later.
After the re-consultation,
The patient asked whether the zygoma reduction method I perform is the so-called "quick zygoma surgery".
"Quick zygoma???"
I have a very negative and skeptical view of quick zygoma surgery.
Quick zygoma does not refer to a specific surgical method; it is simply a general term for methods in which the bone is osteotomized in a short time (15 to 30 minutes) without the surgeon accurately confirming the position of the bone visually, then pushed in by hand and not fixed, or methods that grind the bone through an appropriately small incision.
I have been performing zygoma reduction surgery almost every day for nearly 20 years,
and even when I perform the surgery as quickly as possible while highly experienced, the zygoma reduction surgery I perform still takes at least 1 hour and 30 minutes.
In addition, in October 2012, when the Asian Academy of Aesthetic Plastic Surgery, one of the international plastic surgery societies, was held in Korea, I actually demonstrated a "live surgery on zygoma reduction surgery" at Asan Medical Center in front of domestic and foreign plastic surgeons attending the conference, and answered their questions.
"Sideburn incision area???"
The patient came for a third consultation and asked about the sideburn incision area.
After I explained the position of the sideburn area where I make the incision and the length of the incision, the patient asked why my incision area is so long, since other places say they only make a vertical incision of about 1 cm inside the sideburn.
The sideburn incision area I use in zygoma reduction surgery is
the product of valuable experience, determined as the optimal incision site for maximizing posterior zygoma reduction and ensuring accurate fixation, after I have personally performed thousands of zygoma reduction surgeries over nearly 20 years and observed postoperative progress.
"Is it appropriate not to take a new preoperative CT even though a year has passed since the first consultation???"
After much deliberation, the patient decided to undergo zygoma surgery, and the operation was completed very smoothly and successfully.
However, after surgery, the patient expressed additional anxiety and questions.
The concern was whether it was really appropriate that a CT was taken at the time of the consultation a year earlier, but no CT was taken before surgery.
I had clearly confirmed after the first consultation whether the patient had undergone any surgery in the zygoma or facial bone area, and the patient said that there had been no surgery at all in the facial bone area after the first consultation, so I thought additional CT was unnecessary.
I have great concern that people who are considering or undergoing facial contouring surgery may be exposed to radiation by having unnecessary CT scans.
Therefore, my philosophy is that CT should be avoided unless it is absolutely necessary.
"That there is no CCTV in the operating room???"
Among the people who come to me for contouring consultations, quite a few ask about CCTV in the operating room.
For those who want it, I record the scene of the surgery on my phone.
However, it is true that there are many risks and concerns regarding constant CCTV recording in the operating room.
For example, even in plastic surgery operating rooms, there are many surgeries involving body contouring or simple autologous fat grafting that inevitably proceed with the patient undressed from the waist up or down.
Also, before starting general anesthesia, the process of attaching ECG leads to the chest necessarily exposes the upper body as a whole.
For that reason, I deliberately step away during the process of connecting the ECG leads before starting general anesthesia, or during the process of disinfecting the thigh area in the prone position for autologous fat grafting.
If such processes or scenes were constantly recorded on CCTV and that material were to be leaked by mistake, it could cause very serious problems.
Therefore, for those who request it, I separately record the surgery scene for them, even though it is a bit inconvenient.
Thinking about it, I believe the biggest reason people want CCTV in the operating room is distrust regarding the possibility of proxy surgery.
I think proxy surgery is a system that is generally prevalent in factory-style large plastic surgery clinics with many young doctors.
It is likely that some places operate commercially by hiring young doctors who want to gain experience by performing surgeries at relatively low cost and by setting surgery fees very cheaply.
However, considering the structure of our hospital and the composition of our medical staff, all of the other directors except me each have their own specialty, and our system is one in which I directly consult with and refer patients to the other directors from the consultation stage for surgical areas where I am lacking.
For me personally, rather than conducting consultations, performing surgery is a much happier and more comfortable time.
"In zygoma surgery, are side effects such as sinusitis or inflammation unavoidable???"
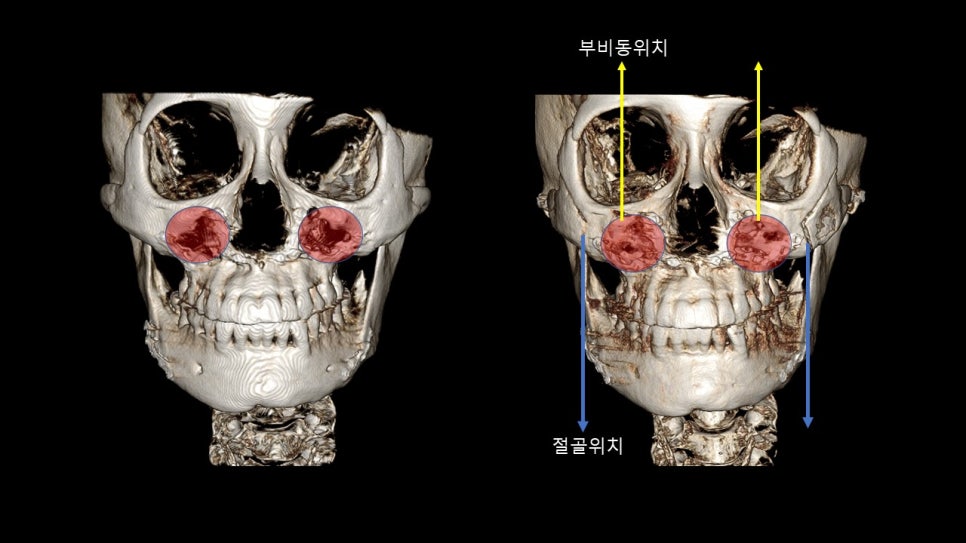
In zygoma surgery, whether the area with the sinus is involved depends on the position and method used to osteotomize the body of the zygoma.
In most surgical methods that remove the body of the zygoma, the sinus is often inevitably exposed,
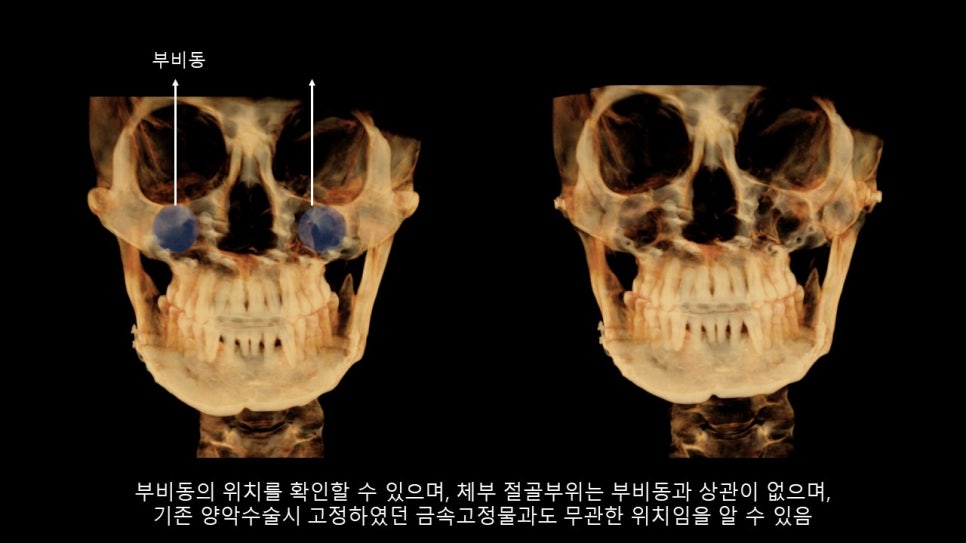
but except in cases of revision zygoma surgery, in the first zygoma reduction surgery I perform, the osteotomy site of the zygoma body is outside the sinus.
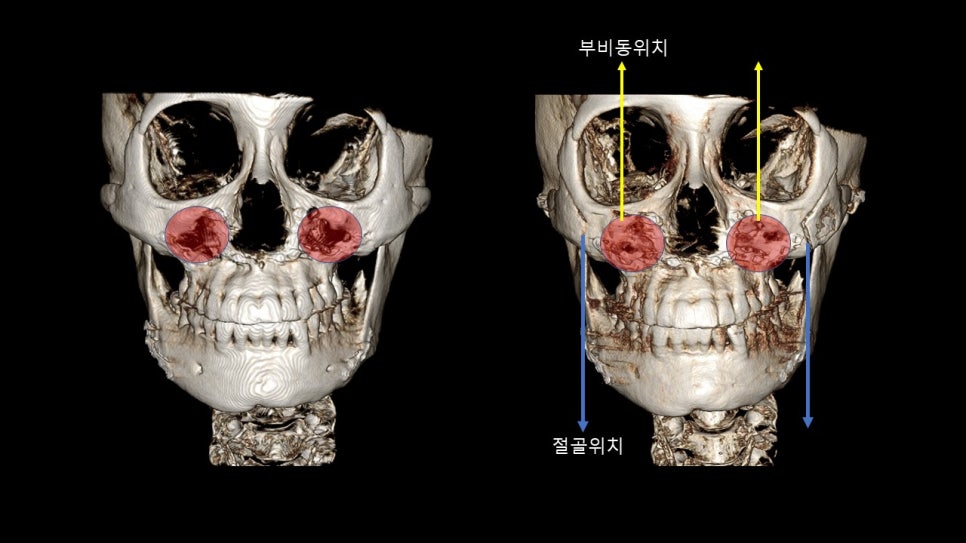
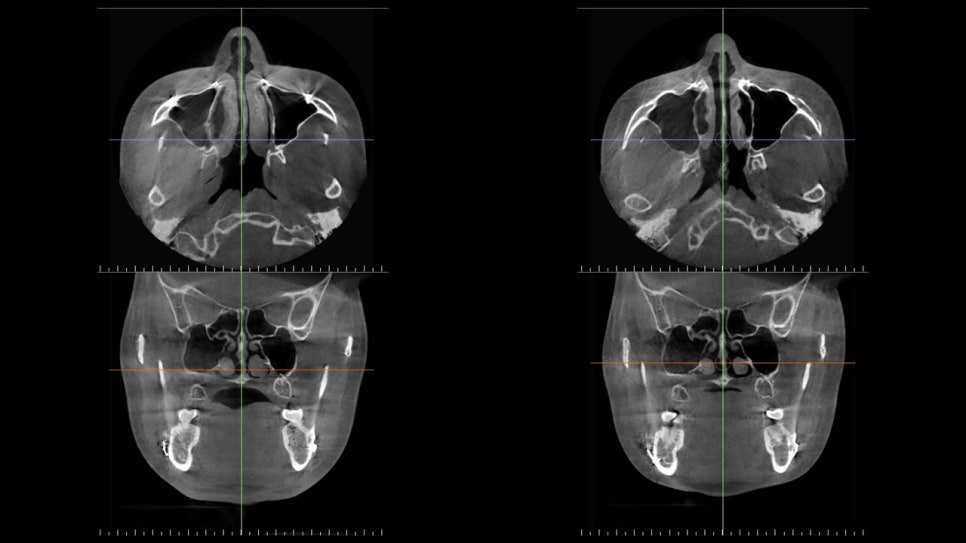
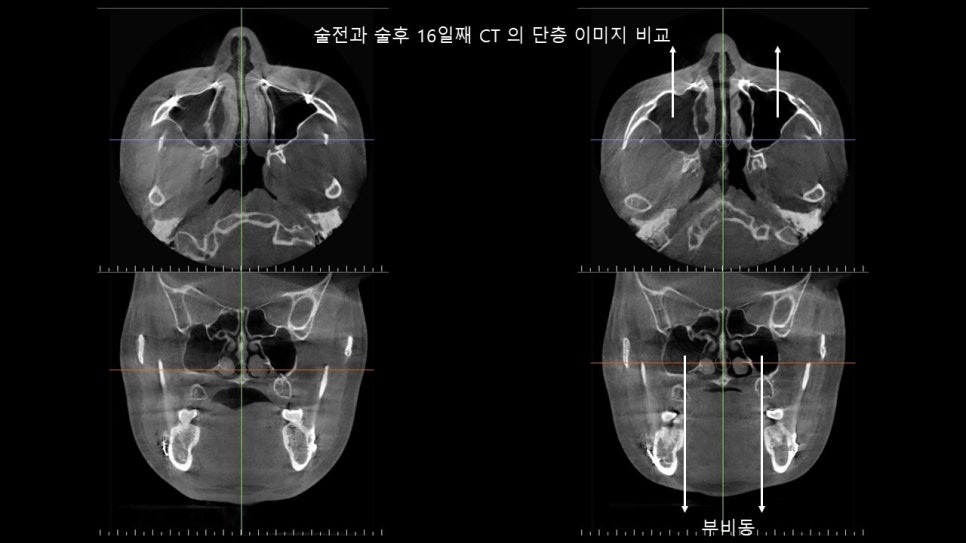
The actual osteotomy site and the location of the sinus can be confirmed on 3DCT, and postoperative CT slices show that the sinus is clean.
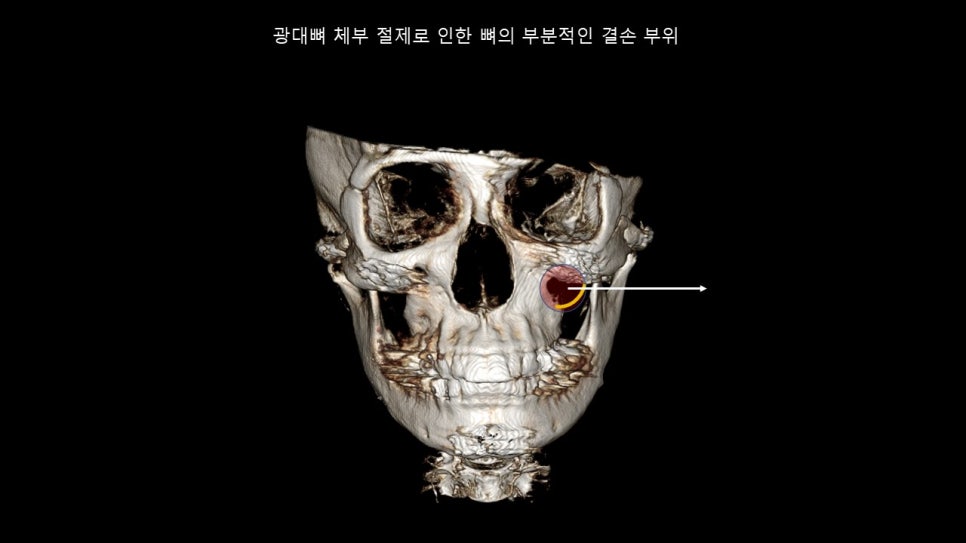
"Concern about cheek sagging???"
The biggest cause of cheek sagging related to zygoma surgery is often due to surgical methods that partially remove the body of the zygoma, where the retaining ligaments are attached.
When surgery is performed in this way, cheek sagging inevitably occurs no matter how much the cut bone is fixed upward, and in the words of those who experienced severe cheek sagging, they lament that "the time and cost spent on lifting surgery to pull the skin back up after zygoma surgery were far greater."
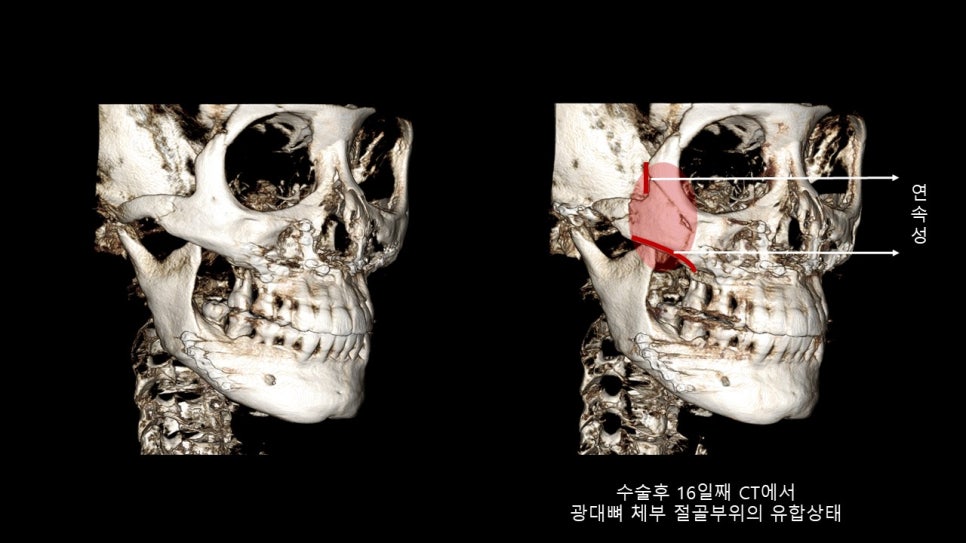
Therefore, I believe it is extremely important to preserve bony continuity when performing zygoma reduction surgery.
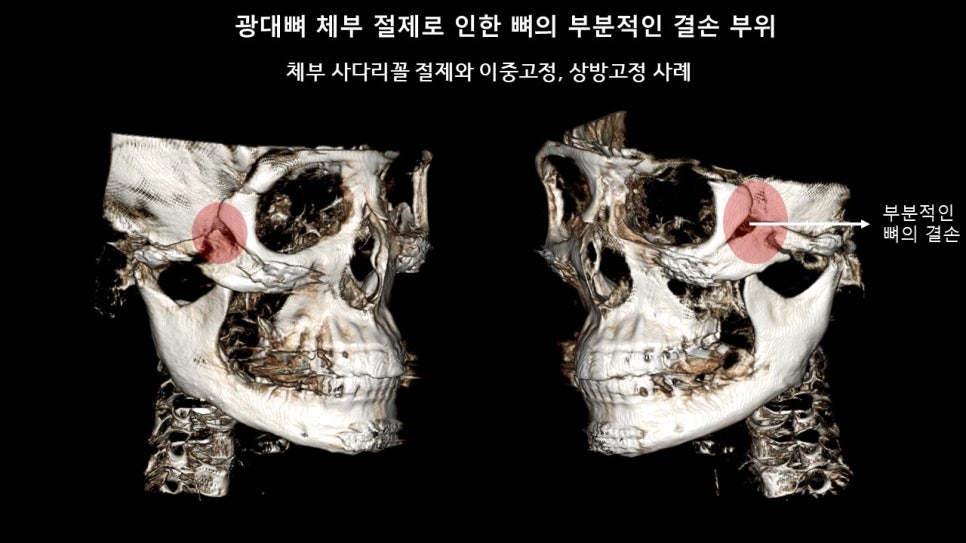
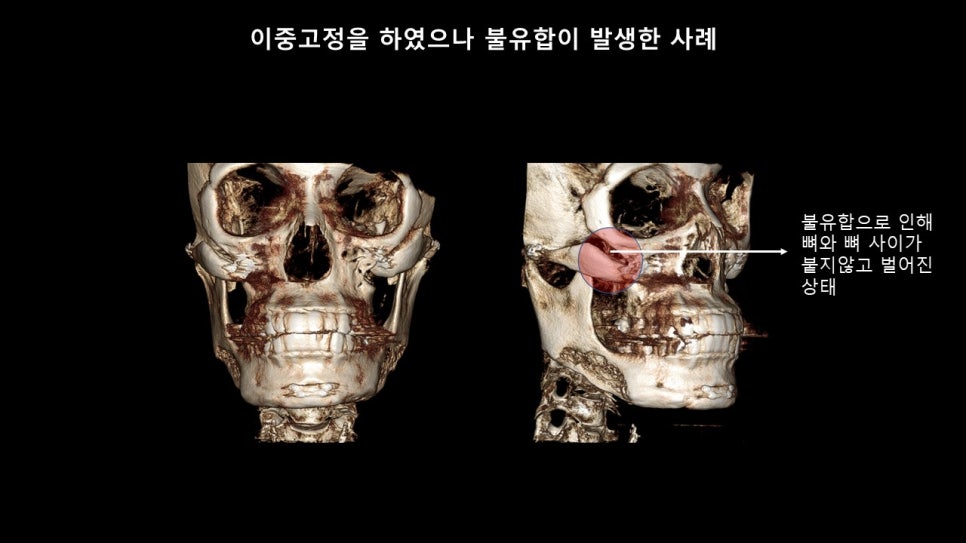
"Nonunion and bone defects???"
A concern that many people have in relation to zygoma reduction surgery is, "What if the bone does not heal properly after surgery and nonunion occurs?ㅠㅠㅠ"
In fact, when both the anterior body, which is the starting part of the zygoma, and the posterior arch area are osteotomized and double-fixed, there is always a high possibility of nonunion or partial bone defects.
Therefore, I understand that many doctors who perform zygoma surgery advise patients to be careful for at least about 3 months after surgery and to avoid chewing very hard foods.
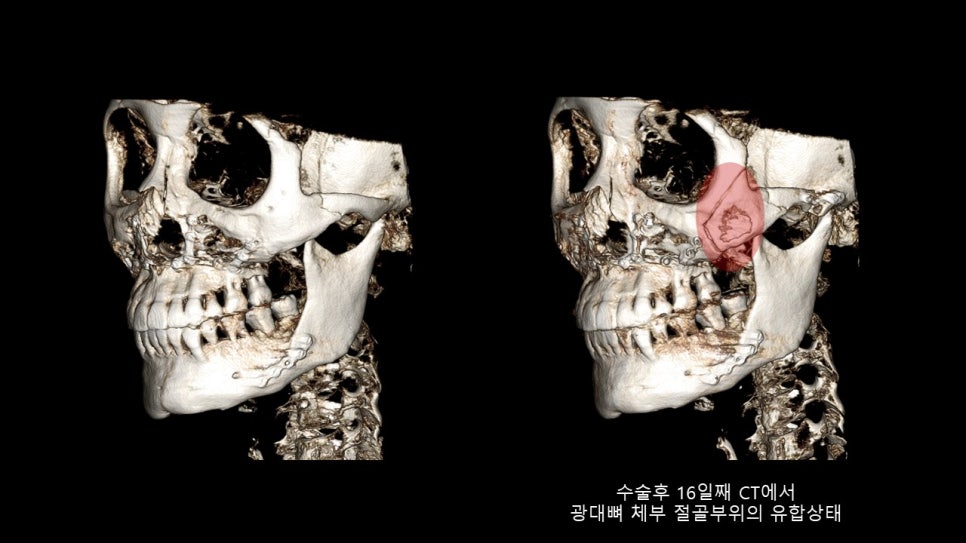
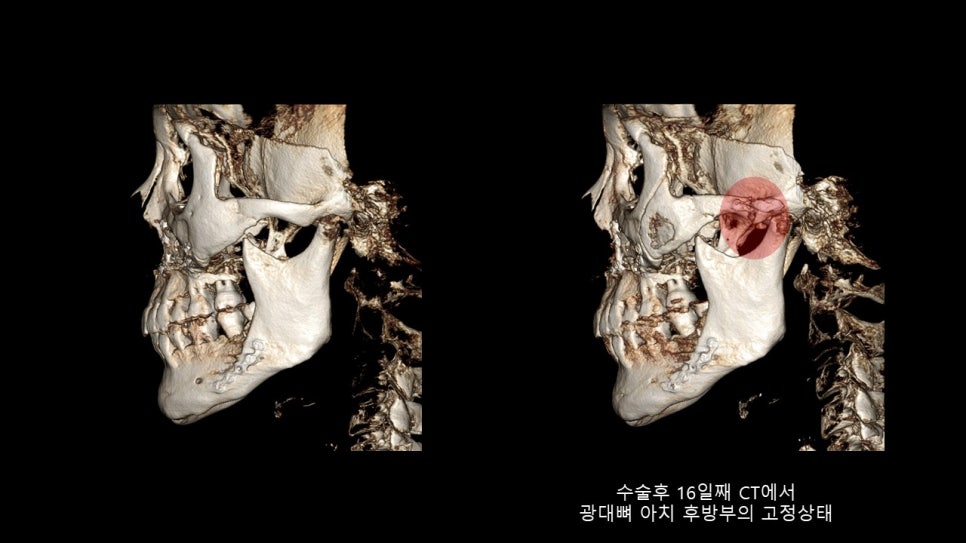
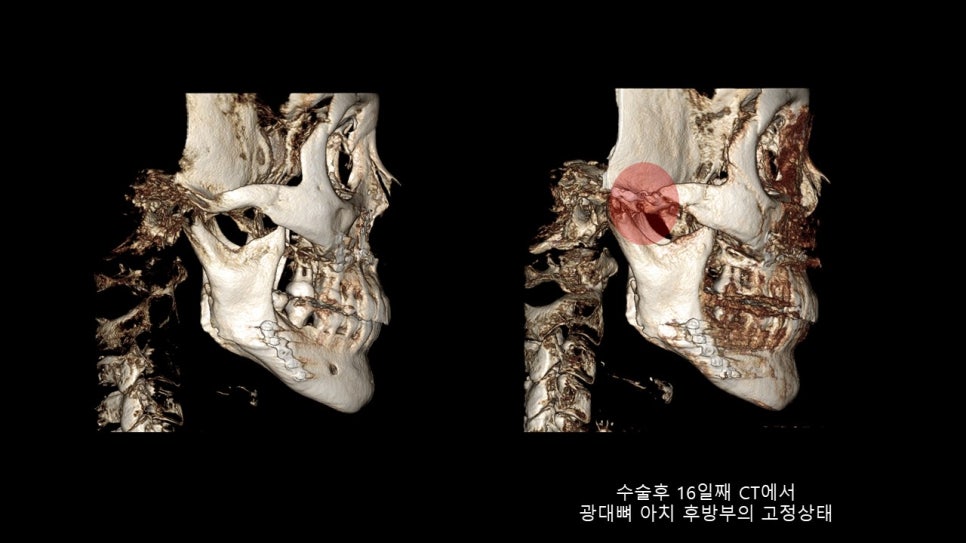
However, in my case, after checking the state of the bone two weeks after zygoma surgery, I recommend returning to daily life as soon as possible and opening the mouth wide and chewing hard foods as well.
When sleeping, even if one casually lies on the side and the lateral zygoma is pressed for a long time, it has no effect on the stability of the bone at the surgical site, and since it is sufficiently stable even against some degree of impact, I urge patients not to worry at all and to go about all of their preoperative daily activities.
There is one part I always emphasize when observing the postoperative progress of people who have undergone surgery with me.
"Unless it is revision zygoma surgery, it is necessary to live comfortably in daily life from two weeks after surgery, and if a problem arises in the operated zygoma area after checking the CT at two weeks postoperatively, then it is my responsibility as the surgeon!"
I am attaching the preoperative and postoperative day 16 CT scans of a patient who worried a lot before surgery and also after surgery^^

In conclusion,
if I summarize my thoughts on postoperative progress and care, they are as follows.
The zygoma surgery method can vary greatly depending on the hospital and the surgeon performing it.
Therefore, the expected results or areas of change from the surgery can be clearly different, and the postoperative care method can also differ clearly depending on the surgical approach.
For postoperative care, it is absolutely necessary to follow the policy and instructions of the surgeon who performed the operation.