Occasionally, most of the pre- and post-operative CT scans from contouring surgeries that I post on this blog are not cases of people who are satisfied after surgery, but rather cases of people who are anxious and unable to trust my explanations.
This is because, for nearly 20 years and thousands of cases that I have personally performed, most of my surgical cases show no major difference, and I have felt that repeatedly posting such pre- and post-operative CT scans would be meaningless.
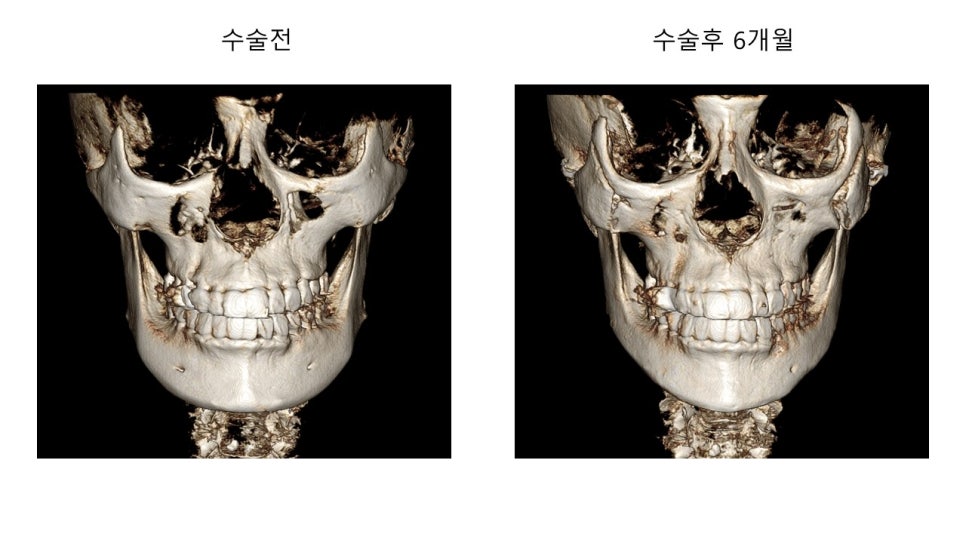
Six months ago, I will explain the direction of the surgery and the union of the osteotomy sites after surgery, based on the changes in the bone appearance before and after surgery in a patient who consulted with me and underwent surgery to improve a somewhat strong-looking chin area and a wide-looking facial shape.
Because the patient had a cute impression, with an overall plump and wide face that looked as if it had a bit of facial fat, and the chin seemed slightly protruded forward with the chin tip and body of the lower jaw standing out, we decided to perform zygoma reduction surgery to reduce the width of the face as much as possible, and for contour improvement of the lower face, we decided to perform a V-line square jaw surgery to smooth the chin tip and the body of the lower jaw as much as possible.
Before surgery, both the zygomatic bone and the lower jaw bone were wider and more prominent on the patient's actual left side compared to the right side, so we planned the surgery with the left side of the lateral zygoma and the body of the lower jaw reduced more.
The patient came for follow-up on postoperative day 5, at 2 weeks, and at 1 month, and after not visiting for a while for follow-up checks, returned at 6 months.
Since the patient came in for a follow-up after a long time, I welcomed them warmly, but from my point of view, what was somewhat absurd was that they had come after being issued a treatment cost estimate for zygoma reoperation from the dental department (oral and maxillofacial surgery) of a university hospital.
Through the following cases, I will compare and analyze the post-operative bone condition of patients who underwent surgery at that dental department and came to me for reoperation consultation.
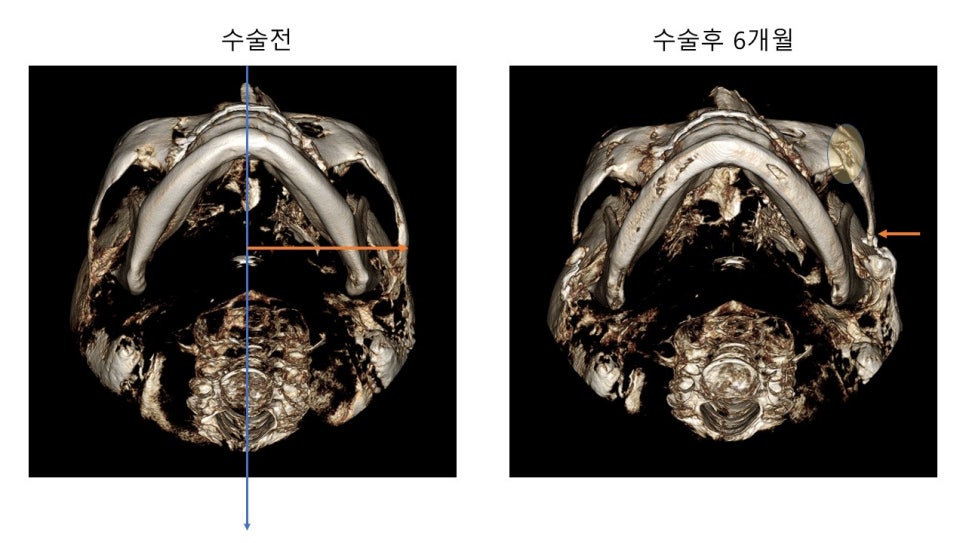
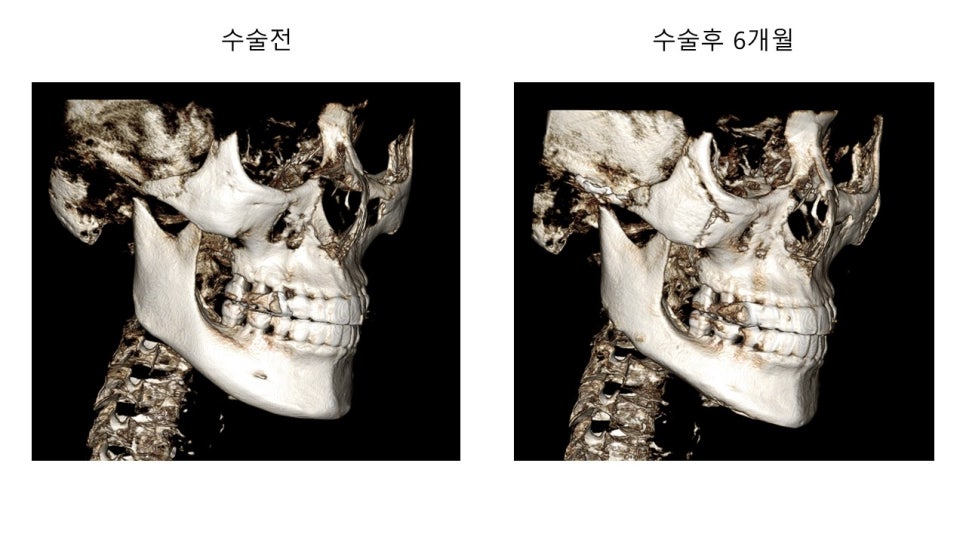
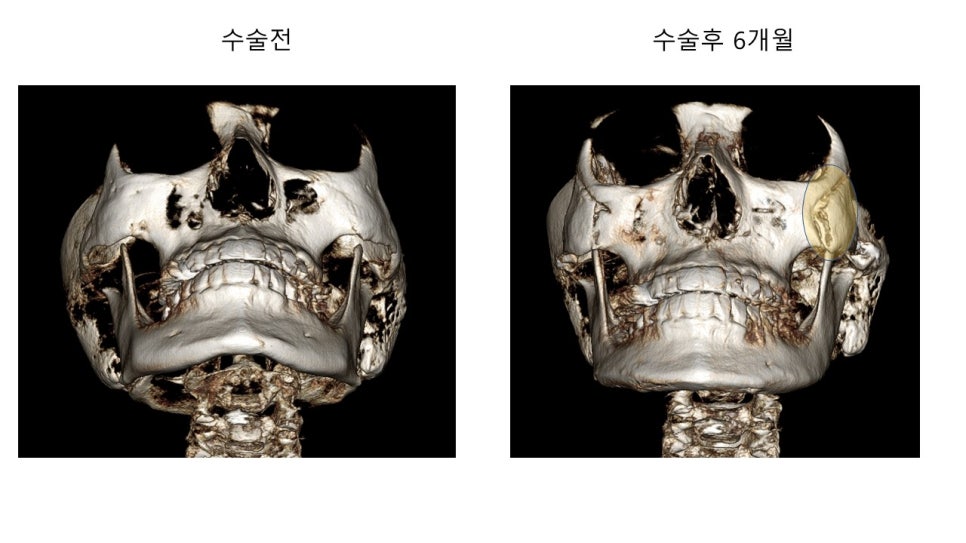
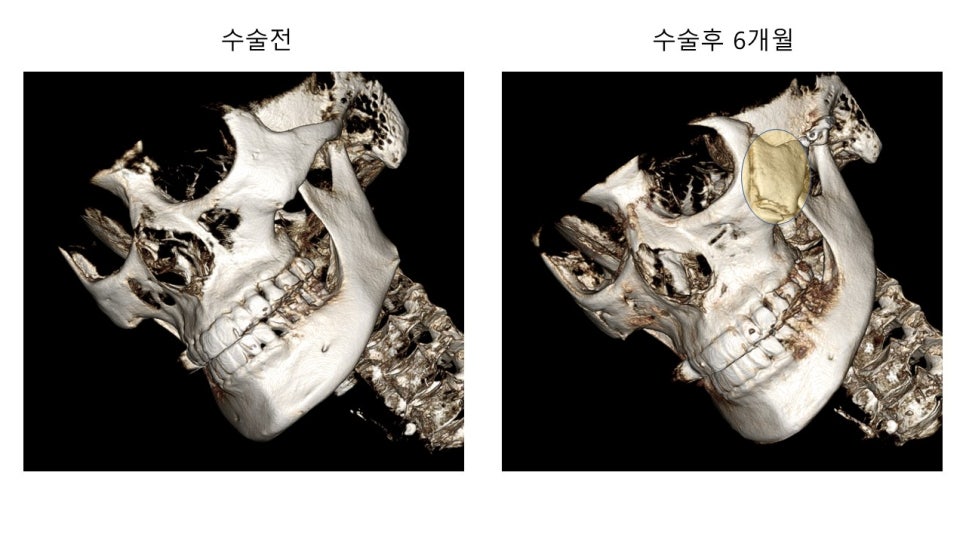
At the 6-month postoperative CT, the patient's actual left side (right side in the photo) showed the osteotomy site opening up, and the patient was anxious about whether it was nonunion.
This is the area marked with a yellow circle in the image below.

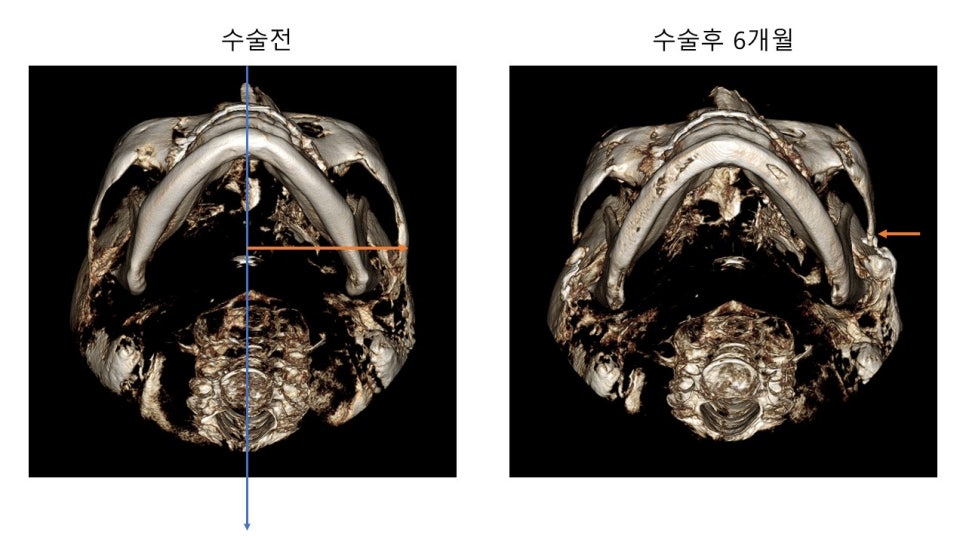
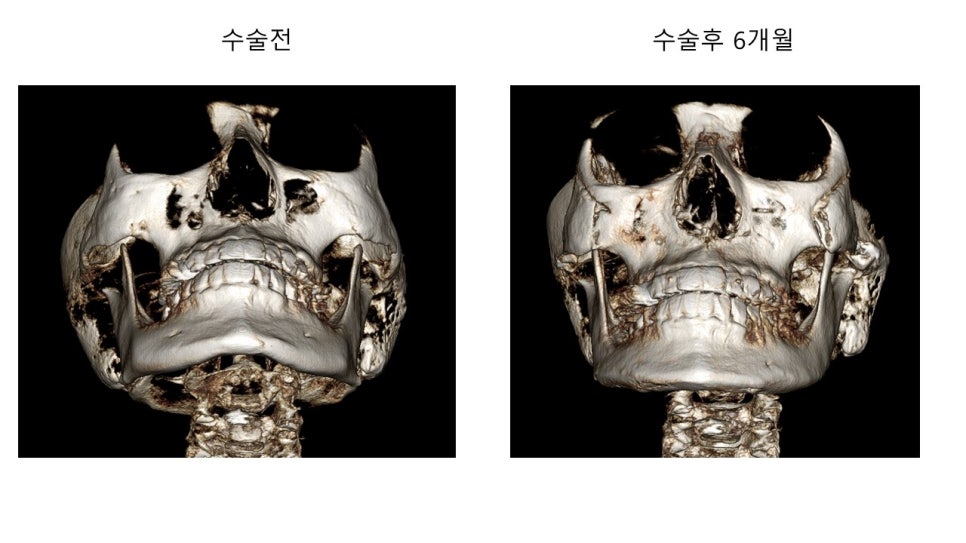
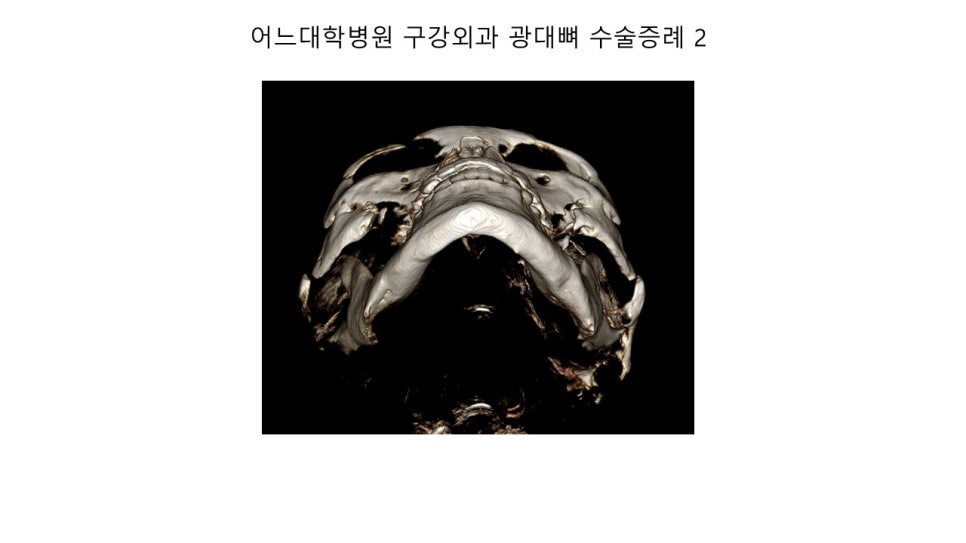
These are CT images from the base view (looking upward from beneath the chin) before and after surgery.
Before surgery, the patient's actual left lateral zygoma and posterior zygoma were wider and more open than the right side, so as shown by the arrows, the left side was moved further inward.
In the CT images viewed from the base before and after surgery, you can see that the union is well achieved.
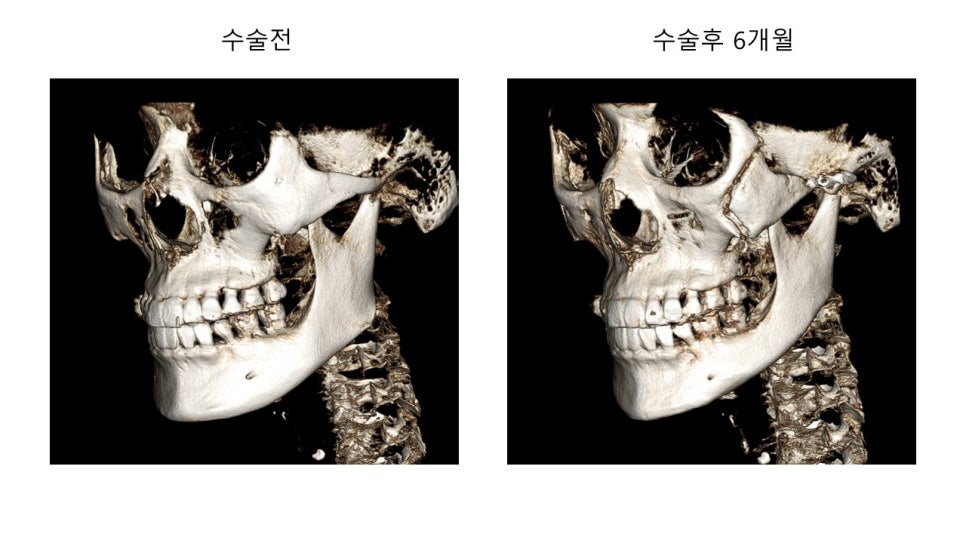
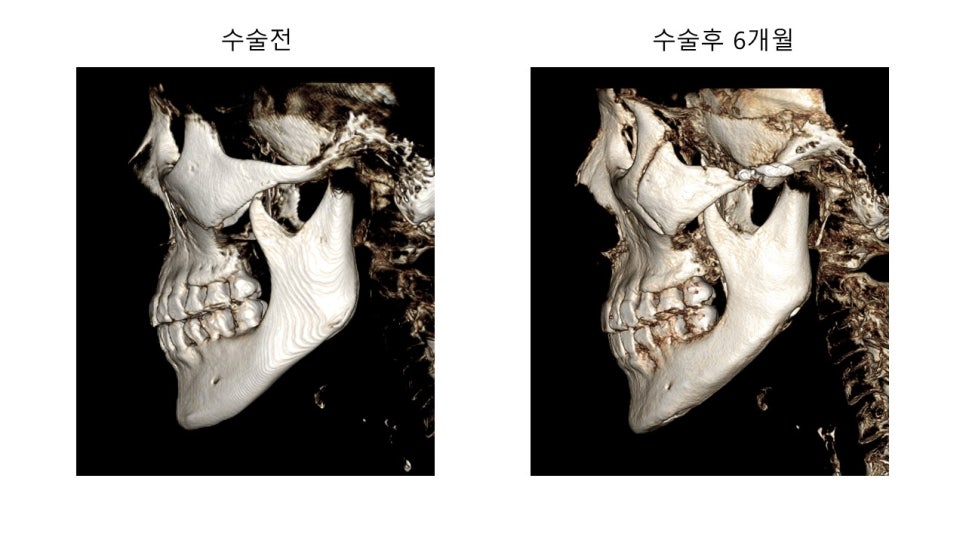
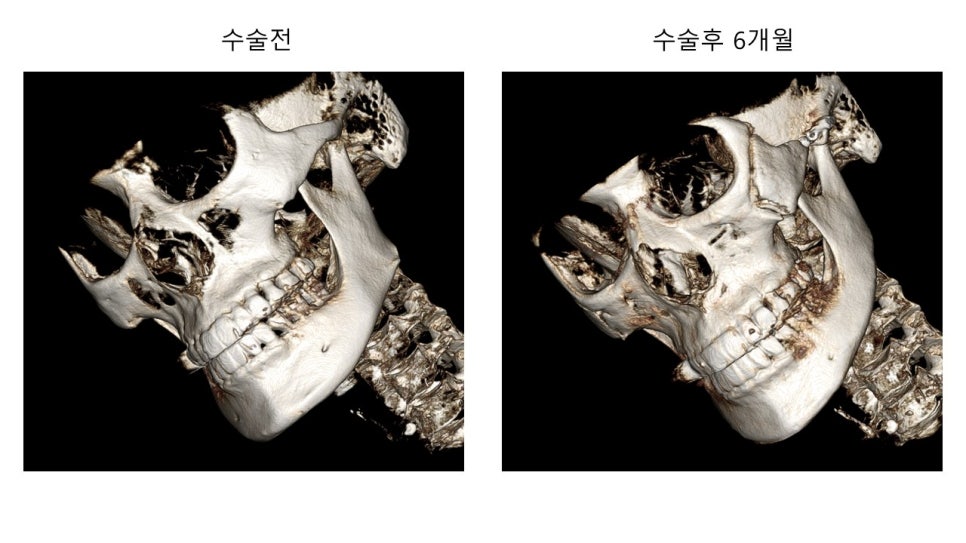
In the postoperative image showing the left oblique view, you can also see that the bone is well united from the upper to the lower part of the osteotomy site, with no gap.
In the CT images viewed from the base before and after surgery, you can see that the union is well achieved.
In the CT images viewed from the base before and after surgery with a slightly changed angle, you can see that the union is well achieved.
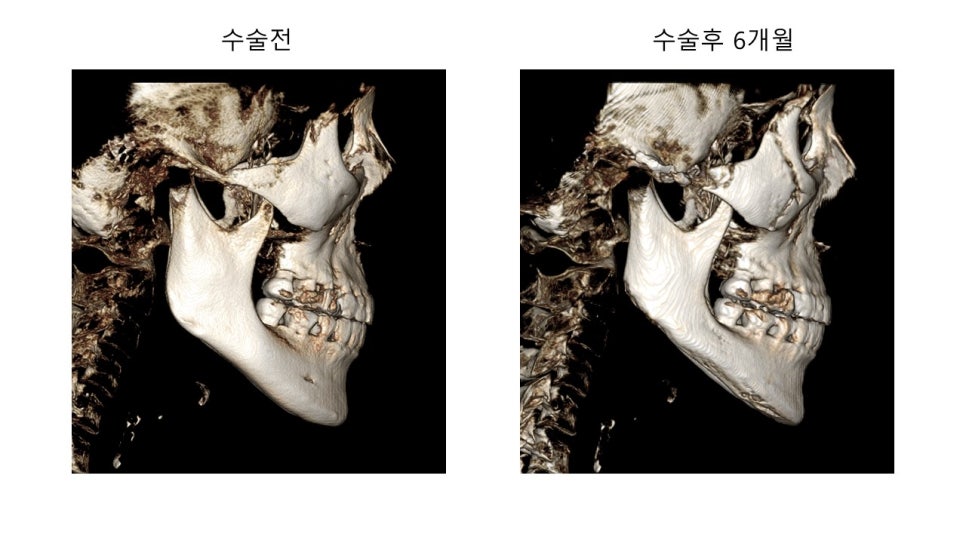
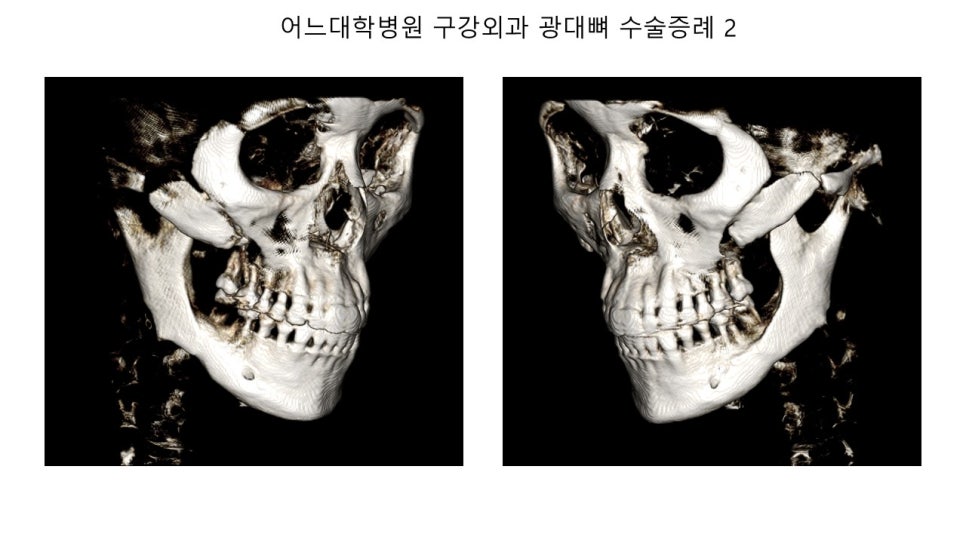
Let's take a closer look at the union status of the osteotomy site from a different angle.
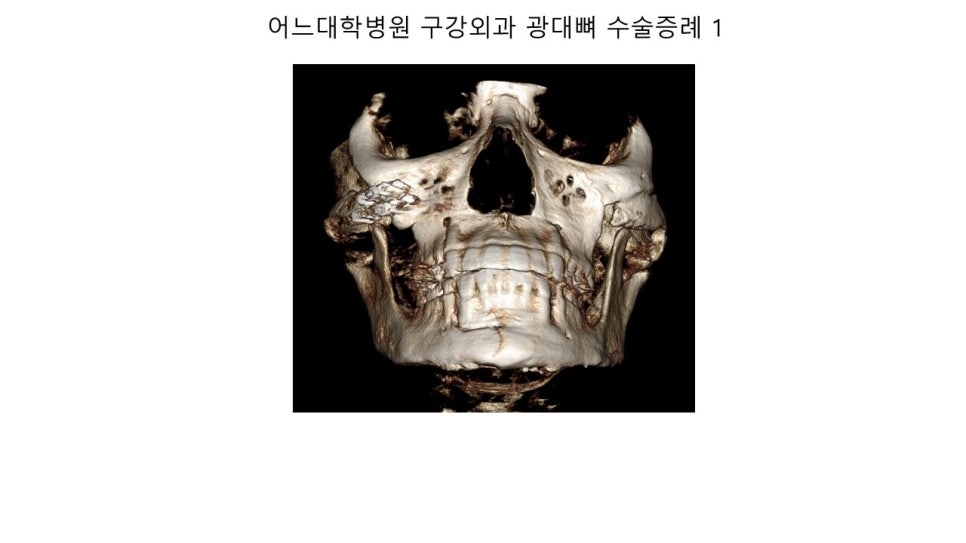
Next, let's look at the cases operated on at that university hospital's oral and maxillofacial surgery department, where consultation for reoperation was provided and a treatment cost estimate was issued.

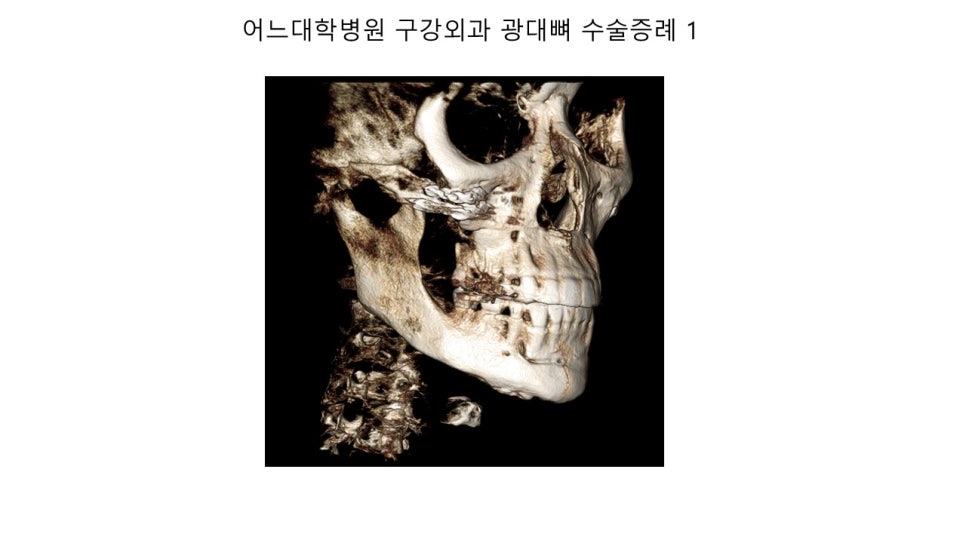
The right anterior osteotomy site has been fixed, but you can see that the bone gap is very large, and in such cases it can actually be diagnosed as nonunion.
This is another case operated on by the oral and maxillofacial surgery department of the same university hospital.
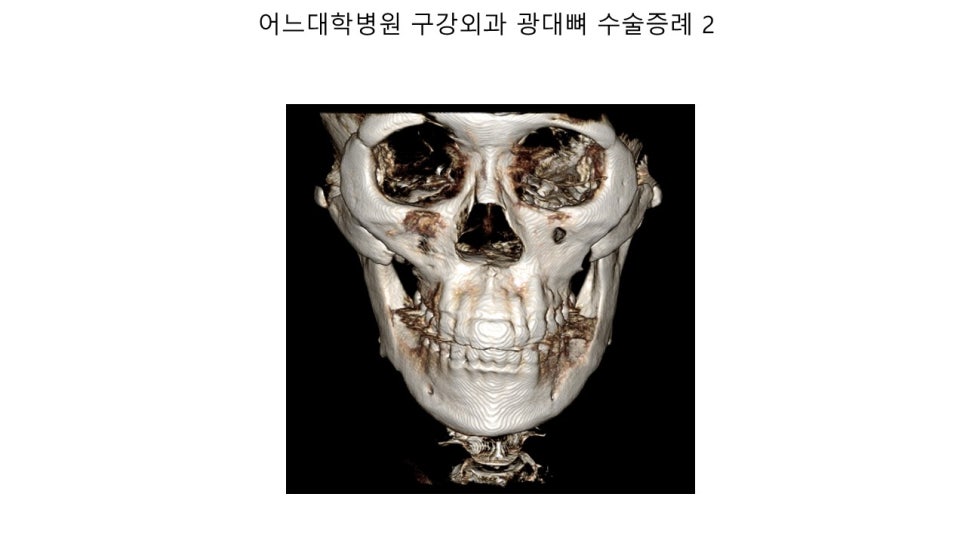
In this case, the anterior osteotomy site has united, but there is a step deformity, and you can see a step deformity around the posterior two-thirds point of the zygomatic arch.
When surgery is performed in this way, the contour of the midface appears flatter and wider than before surgery, and the facial outline appears less smooth because of the step deformity in front of the sideburns.
Also, if the osteotomy is made in an intermediate portion of the zygomatic arch, reoperation can be very difficult.
From my perspective, this is extremely difficult to understand and quite absurd, so I ask for your understanding that I had no choice but to make a post directly comparing and analyzing the cases from that university hospital's dental department (oral and maxillofacial surgery).