People who have received care for hair loss often have the same common experience.
“Each clinic gives a different diagnosis.”
Some places say it is early-stage, some say treatment should start right away, and others emphasize progression in a specific area.
This difference is not simply a matter of physician preference; it occurs because the depth of the diagnostic process, the testing methods, and the interpretation criteria all differ from clinic to clinic.
Hair loss is not a disease diagnosed by a single number, so a more systematic evaluation determines the accuracy of the diagnosis.
Why Hair Loss Diagnoses Differ by Clinic: What Are the Differences?
Summary
-
Hair loss diagnosis is made through a combination of history taking, physical examination, trichoscopy, quantitative testing, blood tests, and interpretation of criteria.
-
Because the depth and method of this process differ from clinic to clinic, different conclusions can result.
-
A good diagnosis focuses on records, comparison, and evidence rather than making a quick conclusion.
-
When patients receive a transparent diagnosis explained with photos and numbers, they can avoid both overtreatment and neglect.
Q1. Why do hair loss history-taking and examinations differ from clinic to clinic?
The first step in hair loss diagnosis is taking a medical history and identifying the pattern.
International reviews also state that a thorough medical history and physical examination are the starting point for diagnosis¹.
However, in actual practice, differences arise in the following ways.
A clinic that asks about stress, sleep, medications, sudden shedding patterns, and family history
- Simple check and then prescription
Hair loss is not just about whether it looks like it is falling out. The key is why, when, where, and in what pattern it appears.
Because this stage must be solid for the later diagnosis to be accurate, it becomes the starting point for why different clinics reach different conclusions.
Q2. Why do trichoscopy results differ even when the same scalp magnification test is performed?
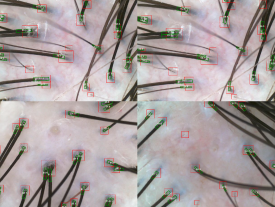
Trichoscopy is known to be an important tool in diagnosing most hair and scalp disorders³.
But using the same device does not mean the interpretation will be the same.
Some clinics use it only to show an enlarged image.
Some clinics carefully assess hair shaft diameter variability, miniaturization, inflammation, and whether follicular openings have disappeared.
Even when looking at the same photo, different eyes lead to different conclusions.
In particular, distinguishing scarring from non-scarring hair loss and determining whether it is progressing are strongly influenced by clinical experience.
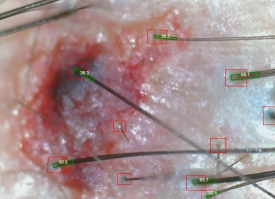
Q3. What is the difference between clinics that perform quantitative tests such as phototrichograms and those that do not?
Quantitative testing shows the condition of hair loss in numbers through data such as the following.
The literature also describes phototrichograms as a key technique that can objectively measure density and hair cycle ratios⁴.
However, in real-world practice,
This difference leads directly to differences in diagnostic conclusions.
Quantitative data is becoming increasingly important because it provides a strong basis for determining the treatment direction.
Q4. Is there a reason blood tests are done differently from clinic to clinic?
Blood tests are not absolutely necessary for every patient with hair loss.
International guidelines also distinguish them as follows.
Male pattern hair loss
Not essential unless there is a special history or symptoms².
Female pattern hair loss
The need for tests such as iron, vitamin D, B12, thyroid function, and prolactin is mentioned⁵.
For some people, detailed blood work is needed.
For some, simple tests are enough.
For others, a clinical judgment can be made without testing.
Because these criteria differ from clinic to clinic, the scope of testing and the diagnosis also differ.
Q5. Does the diagnostic standard for hair loss itself differ from clinic to clinic?

Hair is not a disease determined by a single number.
Diagnosis can differ depending on the following interpretation criteria.
-
How far to consider a natural physiological M-shaped recession as normal
-
From what degree of hair shaft diameter variability to judge it as “progressive”
-
Whether the clinic tends to start preventive treatment early
-
Whether the clinic tends to observe until a clear change is seen
All of these may be clinically valid, but if patients hear only the conclusion without context, confusion can arise.
Q6. What is a good hair loss diagnosis like?
A good diagnosis is not about flashy equipment, but about a systematic process.
-
Record the current hair and scalp pattern with photos and numbers
-
Compare under the same conditions when changes occur
-
Clearly explain the evidence behind the conclusion
-
Do not jump to conclusions too quickly, and do not speak vaguely either
Because hair loss is a condition that changes over years, the initial diagnosis determines the overall treatment strategy going forward.
In the end, the important question is not which clinic to visit, but who explains my hair transparently.
| Category | Difference in approach | Effect on the patient |
|---|
| Depth of history taking and examination | Clinics that ask in detail vs. simple confirmation | The conclusion changes from the initial diagnosis |
| Use of trichoscopy | Interpretation-focused vs. simple image viewing | Difference in accuracy when distinguishing scarring and non-scarring hair loss |
| Whether quantitative testing is performed | Phototrichogram performed vs. visual assessment only | Difference in objectivity when judging before and after treatment |
| Scope of blood tests | Individualized testing vs. uniform testing or omission | Difference in treatment strategy based on test results |
| Philosophy of diagnostic criteria | Prevention-focused vs. observation-focused | Different interpretations of early-stage vs. progressive disease |
Now it is time for hairhair, Kim Jin-Oh.
Pilsaengsinmo (必生新毛).
Written by: Kim Jin-Oh, New Hair Plastic Surgery Clinic (Public Relations Director, Korean Society of Plastic and Reconstructive Surgeons / Academic Director, Korean Society of Laser Dermatology and Hair)
References
- Minta A, Rose L, Kobayashi S, Dulmage B. (2023). Diagnostic Evaluation of Hair Loss: A Narrative Review. EMJ Dermatology.
Quoted: To successfully diagnose and treat patients with hair loss, evaluation begins with a thorough history and physical examination.
- Blume-Peytavi U, Blumeyer A, Tosti A, et al. (2011). S1 guideline for diagnostic evaluation in androgenetic alopecia in men, women and adolescents. British Journal of Dermatology, 164(1), 5–15.
Quoted: In men, laboratory testing for the diagnosis of AGA is unnecessary, except if the history or examination provide clues for another underlying disorder.
- DermNet NZ. (2023). Trichoscopy: A Complete Overview.
Quoted: Trichoscopy represents a valuable, non-invasive and low-cost technique which can be of help in diagnosis of most hair and scalp diseases.
- Brancato S, Cartigliani C, Bonfigli A, Rigano L. (2018). Quantitative Analysis Using the Phototrichogram Technique of an Italian Population Suffering from Androgenic Alopecia. Cosmetics, 5(2):28.
Quoted: The most common technique used is the phototrichogram, which determines hair density and anagen and telogen percentages in a selected scalp area.
- Mohy SM, Ismail MA, et al. (2025). Consensus Recommendations for the Management of Androgenetic Alopecia. Clinical, Cosmetic and Investigational Dermatology.
Quoted: Diagnosing AGA in women may require hormonal testing and blood work for vitamin D, iron, B12, TSH, and prolactin.
[This post is written directly by a board-certified plastic surgeon for information-sharing purposes in accordance with Article 56, Paragraph 1 of the Medical Service Act. Hair loss surgery and treatment may have side effects, and they should be carefully decided upon through consultation with a specialist.]