The hospital that performs upper eyelid fat grafting the most
Word of mouth backed by a reason: Revealing upper eyelid fat grafting know-how
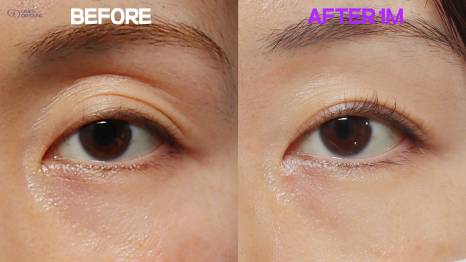
Hello, I’m Dr. Choi Moon-seop, Director of Grace O&Young Plastic Surgery. I can confidently say that our hospital is one of the places that performs upper eyelid fat grafting very often.
Many people leave comments on YouTube and ask a lot of questions. Among them, one of the most frequently asked is [where is the best place for the fat to go when placing fat in the upper eyelid].
Today, I’ll explain that part. When performing upper eyelid fat grafting, fat is inserted with a cannula. *Cannula: a needle with a rounded tip; it is less likely to puncture blood vessels, so bruising and vascular damage are reduced. There are two layers where fat can be placed using this cannula.
The first is below the orbicularis oculi muscle, which is the muscle around the eye.
There is a method of placing it beneath that.
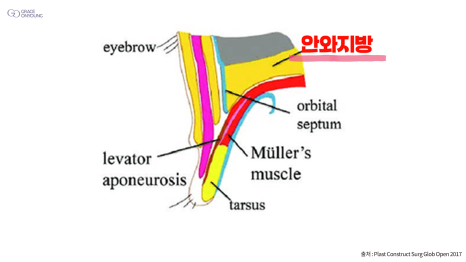
The second is the method of placing it into the orbital fat.
I usually place it into the orbital fat.
The advantage of placing it below the orbicularis oculi muscle is that inserting the fat is easy. Finding that layer itself is not difficult. However, when placing the fat, it must be spread out well so it does not clump together. If that is not done properly, the area where the fat was placed may appear bunched up when you close your eyes or touch it, which is a drawback.
I mainly place it into the orbital fat, and I think placing it there is the most physiologically appropriate. The inner part of the eye is called the orbit, and there is a lot of fat inside it.
Upper eyelid hollowness happens when this fat gradually diminishes. The causes of upper eyelid hollowness can be constitutional or related to family history, but fundamentally, it is due to a lack of fat. So I place it in the orbital fat with the idea of filling the deficient area. The biggest advantage of placing it in the orbital fat is that when the eyes are closed, the fat is not visible from the outside due to the orbital septum, and it can also feel more comfortable when opening and closing the eyes.

I have performed a great many cases so far, and most patients achieve satisfying results. However, the downside is that the process of going through the various septa to reach the orbital fat is somewhat technically demanding and difficult. The main drawback is that the level of difficulty is high when trying to safely place the fat exactly where it is needed.
And as I kept performing this surgery, my own techniques improved over time, and I actually designed a cannula myself for entering the fat. I also developed a tool that helps make it easier to access the orbital fat. Because placing it into the orbital fat has been showing increasingly good results, I mainly choose that area. Going forward,
I will continue striving for safer procedures and better results. Thank you.