Ptosis correction surgery..
If you are interested in double eyelids,
you have probably heard of it at least once.
Strictly speaking, ptosis correction refers to adjusting the strength of eyelid opening.
In other words, by adjusting how much the upper eyelid covers the iris,
ptosis correction can create a clearer eye shape and impression.
There are incision and non-incision methods
for creating double eyelids.
Likewise, ptosis correction also has incision and non-incision methods.
To put it simply, non-incisional ptosis correction
is like pinning and tying the muscle that opens the eyes,
while incisional ptosis correction shortens the length
of that muscle by the desired amount.
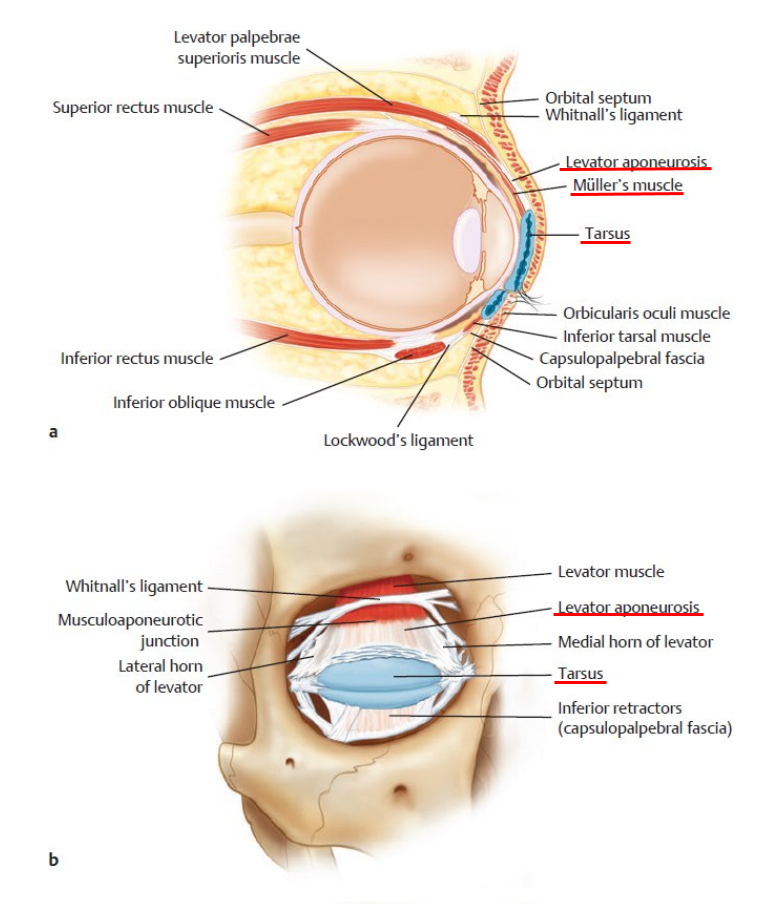
Codner MA, McCord CD. Eyelid and Periorbital Surgery. 2nd ed. New York: Thieme Medical; 2016
I have underlined in red the required terms
in the figure above.
Tarsus: tarsal plate, eyelid plate (the area where the eyelashes are attached; the levator palpebrae superioris and Müller’s muscle are attached here)
Levator aponeurosis: levator aponeurosis of the eyelid
(the part where the muscle that lifts the eyelid attaches
changes from reddish muscle into a white, tough, membrane-like tissue)
Müller’s muscle: Müller’s muscle,
also called the superior tarsal muscle.
The muscle that is tied in non-incisional ptosis correction
is Müller’s muscle.
Müller’s muscle is under sympathetic nerve control,
and it contains a mixture of smooth muscle
(involuntary muscle that cannot be moved at will)
and striated muscle
(voluntary muscle that can be moved at will). [1]
Its width is about 15 mm, and its height is about 10 mm. [2]
This muscle does not play a role at the very beginning of eye opening,
but when the eye is almost fully open,
it helps open the eye about 2 mm more,
and it helps maintain the strength used to open the eye. [2]
So, if the goal is to achieve about 1 mm of ptosis correction effect,
it is possible by tying Müller’s muscle through a non-incisional ptosis correction.
Like this.

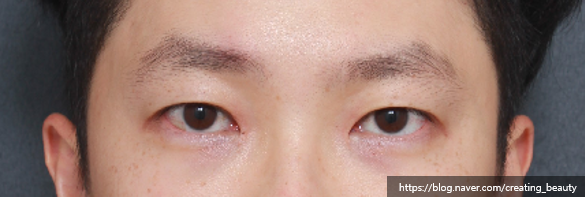
However, when more correction than that is needed,
I recommend ptosis correction through incision.
Cases like the ones below are examples.


It is sometimes said that severe ptosis can be corrected with a non-incisional ptosis correction method by tying up to the conjoint fascial sheath (CFS),
but the amount and result are not easy to predict,
and the discomfort felt by the patient in the eye is also significant,
so I do not recommend the non-incisional method for severe ptosis.
That area cannot be resolved with Müller’s muscle alone.
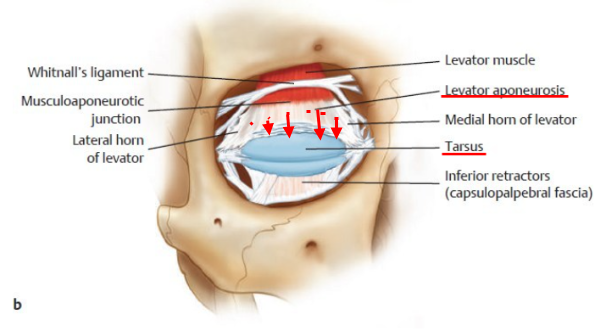
After separating the levator aponeurosis from the tarsus,
the aponeurosis must be lowered by the intended amount and fixed to the tarsus
in order to obtain the desired result.
If the point where the aponeurosis of the muscle that first opens the eye attaches
is here (red dot),
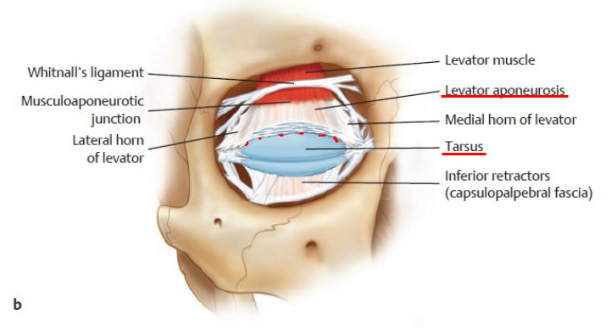
ptosis correction is the process of lowering the aponeurosis above it
and fixing it in place (red arrow).

I hope this helped you understand incisional ptosis correction ^^.
<If you have additional questions, leave a private comment,
and I will kindly answer them. Thank you.>
Reference
-
Bang YH, Park SH, Kim JH, Cho JH, Lee CJ, Roh TS. The role of Müller’s muscle reconsidered. Plast. Reconstr. Surg. 1998 Apr;101(5):1200-4.
-
Beard C. Müller’s superior tarsal muscle: anatomy, physiology, and clinical significance. Ann Plast Surg. 1985 Apr;14(4):324-33.