Lower eyelid fat repositioning, one of the surgeries well known for correcting aging under the eyes, is widely performed on people in their 20s to 40s.
Although lower eyelid fat repositioning is known as a relatively simple procedure, it is performed close to areas related to eye function, such as the eyeball and extraocular muscles, so it requires delicate anatomical knowledge and precise surgical technique.
'Lower Eyelid Fat Repositioning to Prevent Bleeding and Hematoma'
The area under the eyes has a very rich distribution of blood vessels.
If a blood vessel is injured during surgery, bleeding can occur and obscure the surgical field, and bruising or swelling after surgery may last longer and recovery may be delayed.
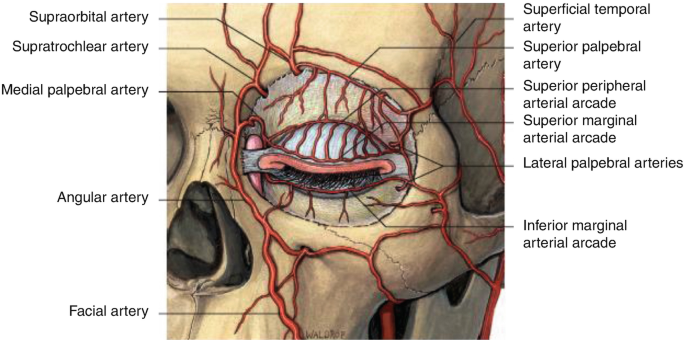
Blood vessel distribution around the eyes.
When dissecting around the tear trough, it is important to minimize bleeding, but because blood vessels are also distributed inside the lower eyelid fat pad, it is important to preserve these vessels while repositioning the fat.
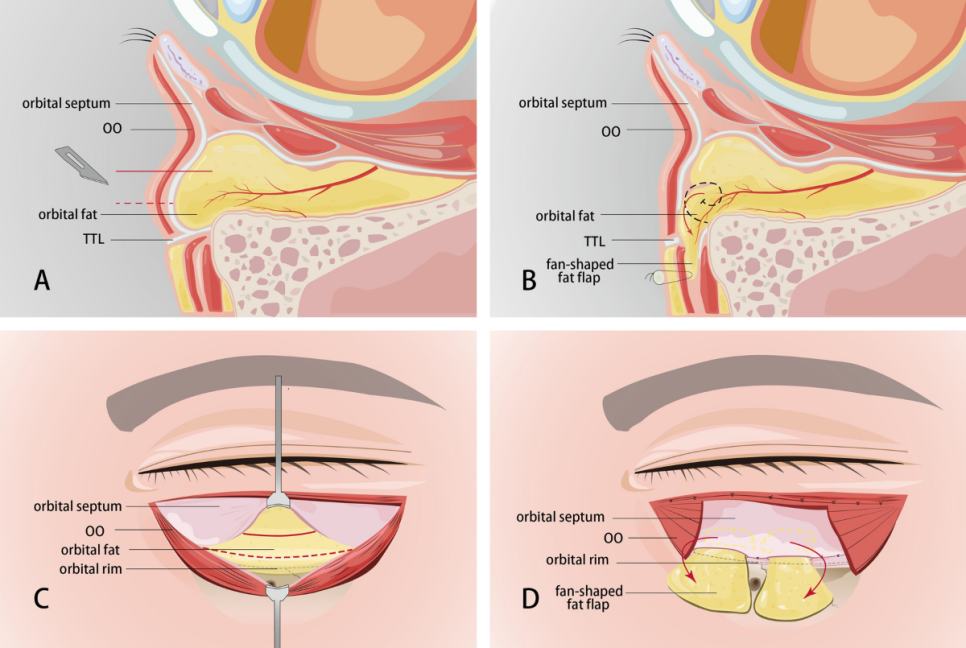
Blood vessel distribution inside the lower eyelid fat pad. Flap-type lower eyelid fat repositioning. Source l Aesthetic Plastic Surgery
The method of moving fat while preserving the blood vessels inside the lower eyelid fat pad is called flap-type lower eyelid fat repositioning. When fat is moved in this way, blood flow in the fat pad is maintained, which has the advantage of making the surgical outcome more predictable and longer lasting.
'Lower Eyelid Fat Repositioning to Prevent Tissue Damage'
There are various surgical instruments that can be used for lower eyelid fat repositioning. Representative examples include the following devices.
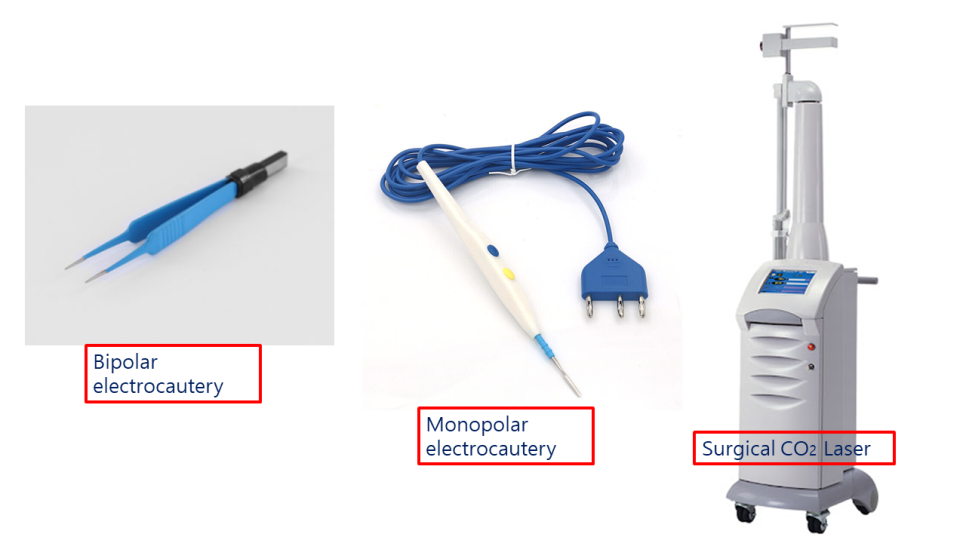
Surgical instruments that can be used for lower eyelid fat repositioning. Bipolar electrocautery. Monopolar electrocautery. Surgical laser.
Among these, the device with the least thermal damage to tissue due to its surgical characteristics is the bipolar electrocautery device, and it is the most commonly used in cosmetic eye surgery.
Less thermal damage means a lower risk of injuring major structures at the surgical site, especially major structures such as the inferior oblique muscle and the Lockwood ligament.
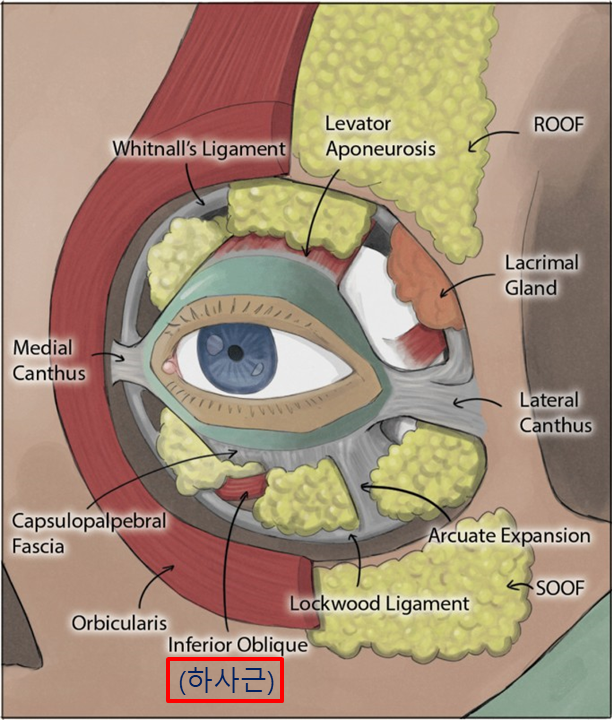
Lower eyelid fat and the inferior oblique muscle. Lockwood ligament.
The inferior oblique muscle under the eye is one of the extraocular muscles, and during lower eyelid fat repositioning, if it is injured or if its movement is restricted by bleeding or swelling, strabismus or diplopia may occur.
Therefore, it is important to perform the procedure using equipment that causes as little tissue damage as possible, while also preventing bleeding appropriately and ensuring that movement restriction of the inferior oblique muscle does not occur during the fat repositioning process.
'Lower Eyelid Fat Repositioning to Protect the Cornea and Eyeball'
Because lower eyelid fat repositioning approaches the lower eyelid through the conjunctiva, the cornea and eyeball must be protected safely during surgery.

Corneal protection device. corneal protector.
If the cornea is damaged by surgical instruments during surgery, discomfort, a foreign body sensation, or changes in vision may occur.
Therefore, it is important to proceed with surgery while protecting the cornea in an appropriate manner.
When lower eyelid fat repositioning is performed in this way, the surgery can be carried out while minimizing bruising and swelling, and safe lower eyelid fat repositioning can be performed by avoiding unwanted side effects such as strabismus, diplopia, and vision damage.

Lower eyelid fat repositioning, aegyo-sal fat grafting, on the day of surgery. This is a partial model who consented to disclosure.
Lower eyelid fat repositioning, aegyo-sal fat grafting, on the day of surgery. This is a partial model who consented to disclosure.

Lower eyelid fat repositioning surgery review. 9 months after lower eyelid fat repositioning surgery. Before and after lower eyelid fat repositioning. This is a partial model who consented to disclosure.