After breast reduction surgery, the issue that troubles patients for a long time is the “scar.”
If we briefly summarize the breast reduction surgery process, it ultimately comes down to excision and a long suturing process.
So breast reduction surgery inevitably comes with the issue of scarring.

That is why people try to fade these scars through various aftercare methods such as scar ointment, silicone gel, scar injections, and laser treatment, but it is difficult to erase scars as if using an eraser.
For that reason, it is very important to make efforts from the beginning to leave scars as short as possible and, even if they inevitably become longer, to leave good scars that are faint in color, flat, and do not rise up.
The scars from breast reduction surgery can be broadly divided into three types.

The three representative areas are the areolar scar, the vertical scar, and the inframammary fold scar.
It would be ideal if all three of these scar areas could be left as good scars, but in reality, it is difficult to leave all three areas as good scars.
The suturing process in surgery is not a flat process but a three-dimensional one, and in such a three-dimensional suturing process, differences in length arise between the two sides of the suture line.
In the end, there is no choice but to close that length difference by gathering it together somewhat in one area.
Therefore, in the case of scars in areas where this length difference is resolved, the results are relatively less favorable than scars in other areas.
Among these three areas—the areola, the vertical line, and the inframammary fold—which scar should be left as a less noticeable, better scar?
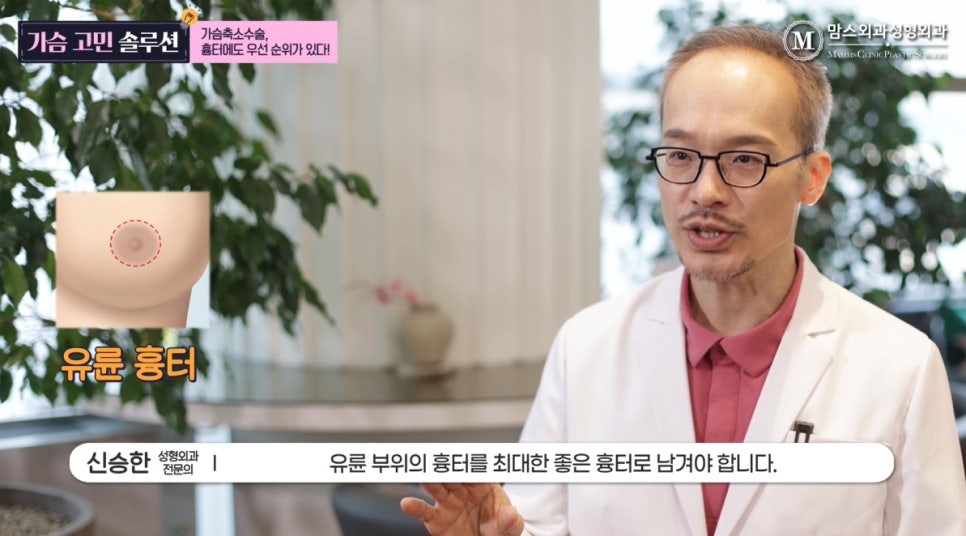
Of course, the areolar scar, which protrudes the most and is easiest to notice, should be left as a good scar.
Next, the vertical line area, which is noticeable from the front, is also important. In the end, the inframammary fold scar, which is located lower and is relatively easier to hide from view, is less important in terms of priority.
Therefore, it is reasonable to distribute the difference in length between the bilateral incision lines in the inframammary fold area and suture them.
However, unfortunately, these days there are increasing cases in which most of the difference in incision-line length is handled in the areolar area, which should remain as a less noticeable scar.
As a result, over time, the areolar scar becomes wider or takes on a large, drooping shape like panda eyes, and these patients often consider revision surgery.
But why is the scar in the most noticeable areolar area left in the worst possible shape?
The reason is the before-and-after photos used in various media and advertisements.
For review-related reasons, all of these media or advertisement photos mosaic the areolar area in the before-and-after images.

As a result, the scar in the most important areolar area becomes an area that is not important for the sake of the photo.
Therefore, most of the difference in length between the bilateral incision lines is shifted around the areola, and the difference in length between the areola and the surrounding skin is finished by suturing in a way that tightens it like the opening of a drawstring pouch.
When the incision lines are sutured around the areola in this way, the scars along the vertical line and the inframammary fold appear short and clean.
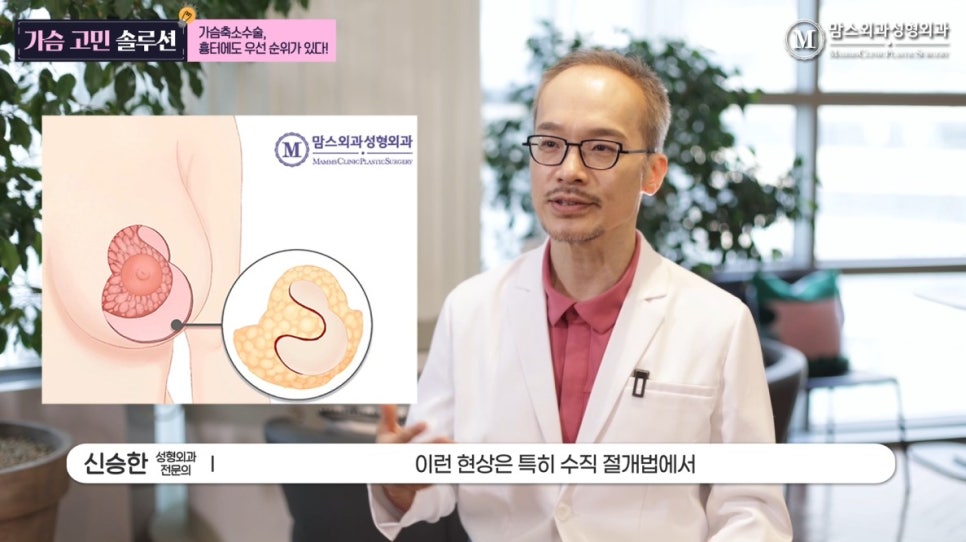
This phenomenon is becoming especially more pronounced in vertical incision methods.
That is because, by shifting as much of the incision-line length difference as possible around the areola and gathering it there, one can eliminate the representative drawback of the vertical incision method—namely, the wrinkled scar that appears below the vertical line.
Instead, the trade-off is that the areolar scar becomes wrinkled.
After surgery like this, it is claimed that the wrinkles around the areola gradually disappear.
However, it was not the case that all of the pioneers who introduced the vertical incision method were foolish and stitched the area below the vertical line in a lumpy way.
All of them were trying to follow the basic principle that the areolar scar should be the least noticeable, so when suturing the areola, they made efforts to ensure that there was no difference in length between the two incision lines.
As a result, wrinkles or poor scars below the vertical line were inevitably difficult to avoid.
There is also a priority when it comes to scar areas in breast surgery.
The most important area is the areola.
Just because it is covered with mosaic in photos and the areola is not visible in pictures does not mean that this scar is not visible in real life.
Keeping the scar in the areolar area as less noticeable as possible is the basic principle of breast reduction surgery.