Inverted nipple surgery is often known as a procedure with a high recurrence rate.
I think this expression is half right and half wrong.
If the milk ducts are preserved, the recurrence rate is high,
and if the ducts are not preserved, the recurrence rate is very low, around 1/1000 to 1/10000.
The reason is the anatomical structure of inverted nipples.
The milk ducts are the passage through which breast milk comes out.
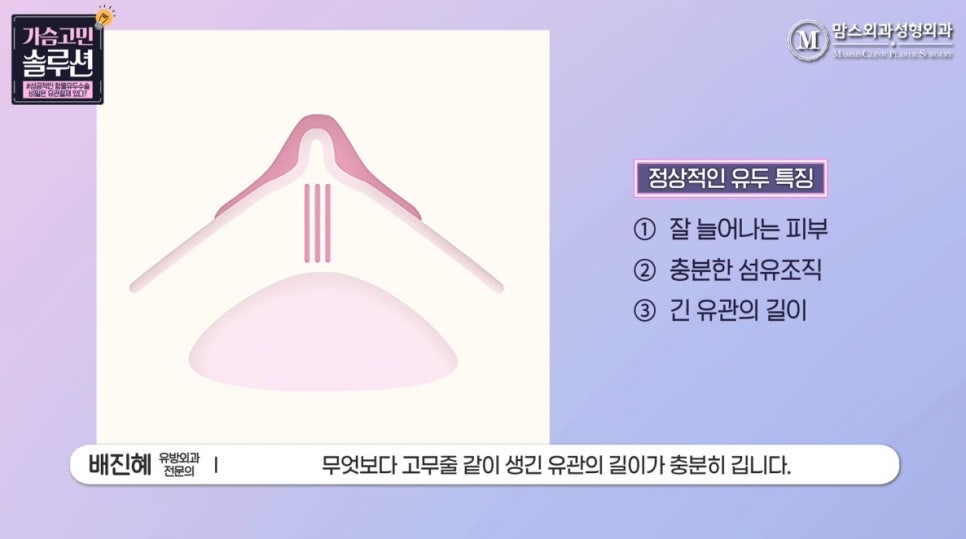
A normal nipple
has skin that stretches well,
sufficient fibrous tissue inside the skin that forms the nipple shape,
and, above all, milk ducts that are long enough, like rubber bands.
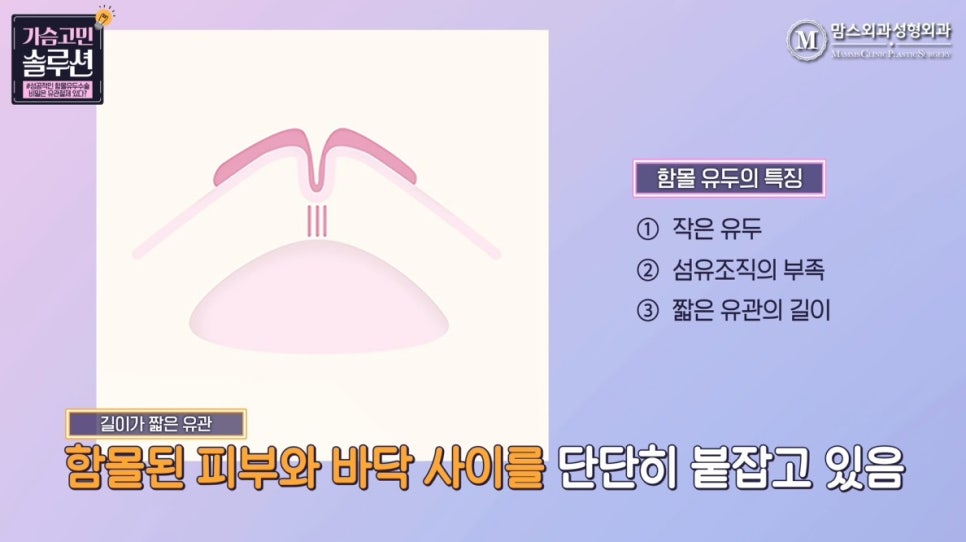
On the other hand, an inverted nipple
often has a small nipple itself.
It also lacks firm fibrous tissue inside,
and, above all, the milk ducts are very short,
which firmly hold the inverted skin and base together.

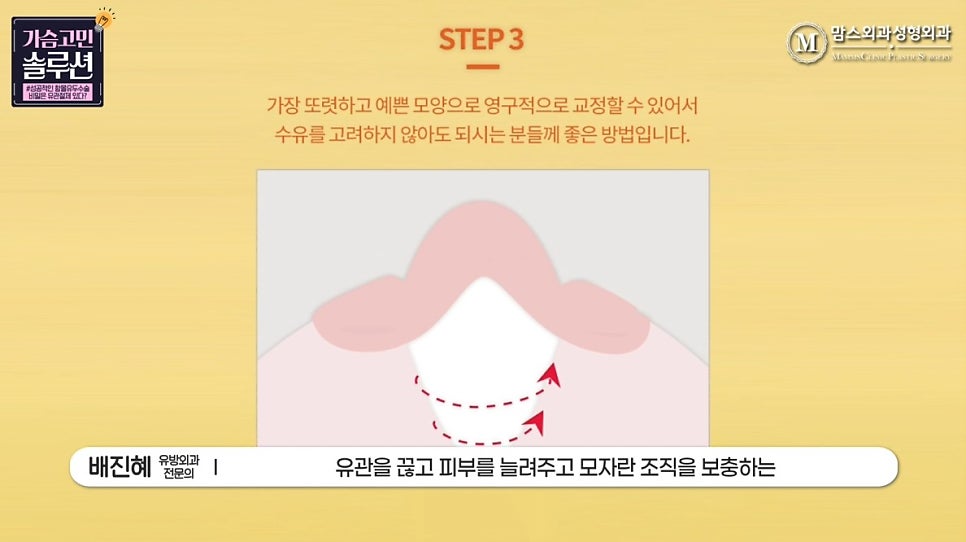
Therefore, if you want to make the sunken or split area protrude,
it cannot be made to protrude unless the milk ducts are cut.
That is what inverted nipple surgery can be said to be.
Among patients with inverted nipples,
some choose the embedding method after hearing that it is simple and that breastfeeding is possible.
In the end, many people return because of recurrence and consult about revision surgery.
Even if some correction is achieved with the embedding method,
a closer look often shows that the nipple still remains in a split shape.
Everyone wants to avoid pain and risk with the least amount of effort possible.
If possible, both medical staff and patients want to preserve the milk ducts using the simple embedding method.
But...
Even if inverted nipple surgery is a minor procedure,
is it really right to correct it with an unstable method that often recurs?
The embedding method can proceed stably
only when the inversion is so mild
that surgery is not even necessary.
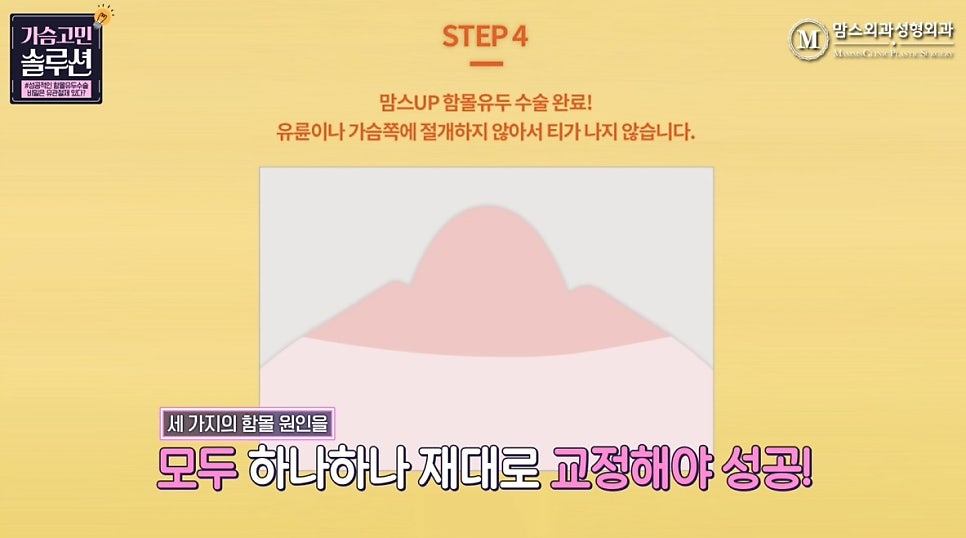
If you want to correct severe inverted nipples without recurrence,
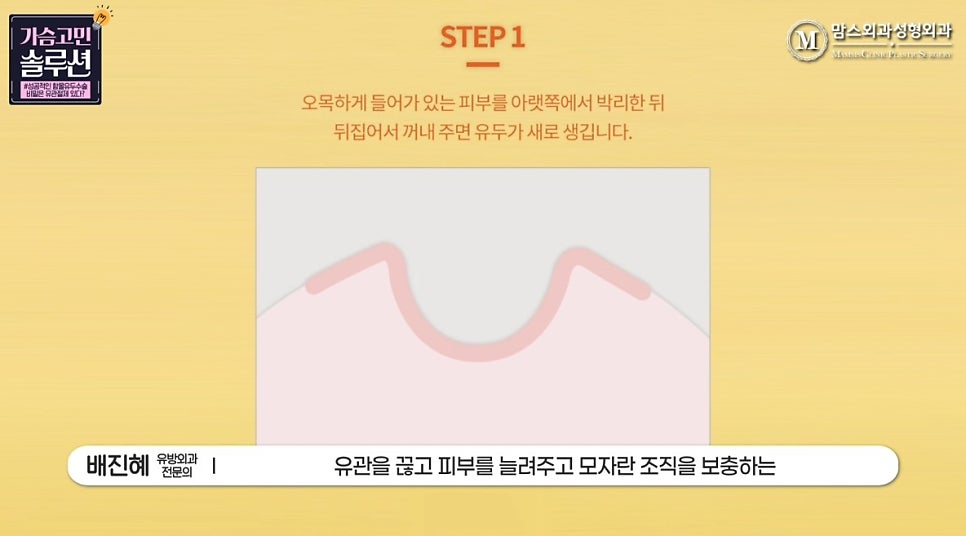
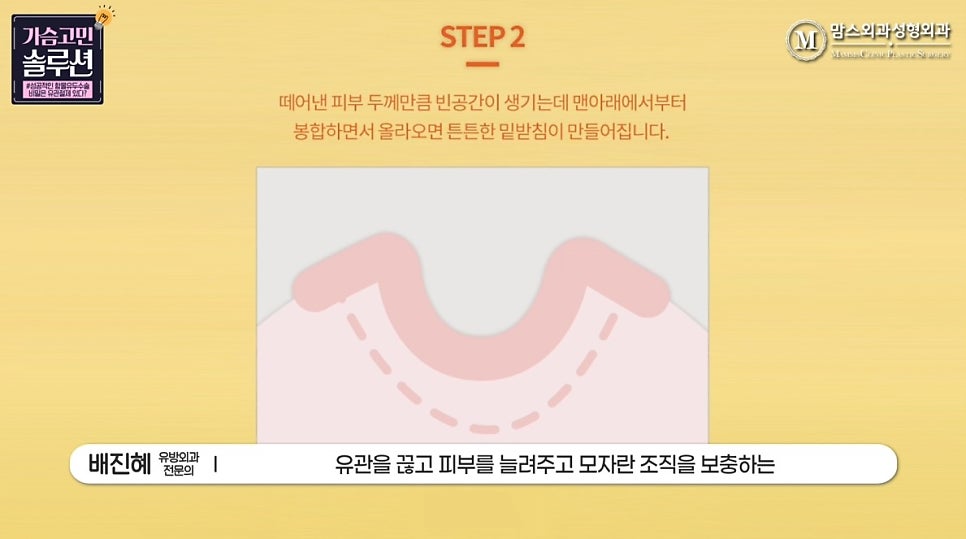
you need to properly correct all three causes of inversion one by one:
cut the milk ducts, stretch the skin, and replenish the lacking tissue.
That is what makes it possible.

When recommending an incision method to married patients,
some worry that it will leave a lot of scars and consider the embedding method instead.
However, even the incision method can show large differences in scarring depending on the surgical technique.
An incision method that approaches from the areola side can leave a noticeable scar,
but if only the split part of the nipple is incised, there is almost no scar left.

The key to success in inverted nipple surgery can be said to be cutting the milk ducts.
The inverted nipple surgery I recommend is this:
for unmarried patients who definitely want to preserve breastfeeding function,
I recommend the incision method that cuts the milk ducts after childbirth
and restores the nipple shape.

For married patients,
it would be good to correct it with the incision method,
which can be corrected with a single surgery.