More people than you might expect are curious about #medialepicanthoplastyrevision. They wonder which method is better and which plastic surgery clinic is best. Because they are investing a lot of money and time, they feel that they cannot afford to fail again like they did with the original medial epicanthoplasty. In fact, for this kind of revision reconstruction, many people feel as if they are grasping at straws, so they ask around on famous online communities or plastic surgery apps. But brokers who take advantage of that mindset are active on every community and every app, and as a result, plastic surgery communities and apps are no longer very helpful.
For those who are curious about medial epicanthoplasty revision, I have organized the information clearly below.
Now, let’s look at the various surgical methods for medial epicanthoplasty revision. These can roughly be divided into three methods.
-
V-Y advancement flap
-
Z-plasty
-
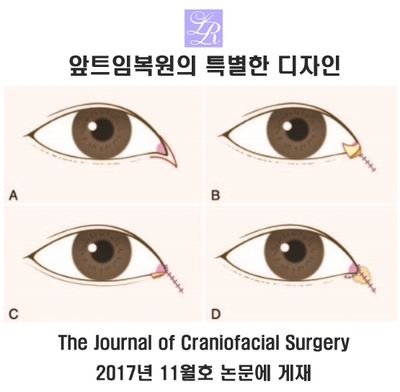
turnover reverse rotation flap repositioning
Other methods such as reverse skin flap repositioning or double flap adjustment can be considered variations of the V-Y method or Z-plasty.
The V-Y advancement flap is the origin of medial epicanthoplasty revision because the design is simple: an incision is made in a V shape and then brought together and sutured in a Y shape. Z-plasty uses a slightly more complex design. Since the V-Y method has the drawback of reopening easily and recurring due to skin tension, Z-plasty is a method that disperses that tension. The design differs, but in the larger picture, both methods share the common feature of pulling in surrounding tissue to reconstruct the area.
Pulling tissue in means forcibly drawing in tissue that does not naturally move, so it has a tendency to pull back toward its original position. This tension can be especially problematic in medial epicanthoplasty revision because only the outer skin is forcibly pulled in, leaving the back side of the reconstructed epicanthal fold almost empty. That can increase the recurrence rate, which is why V-Y and Z-plasty have those limitations.
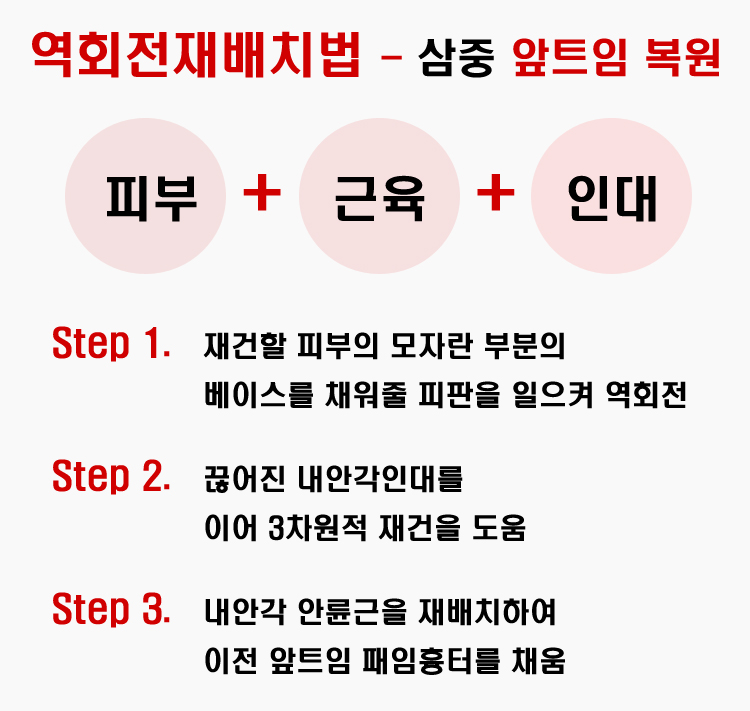
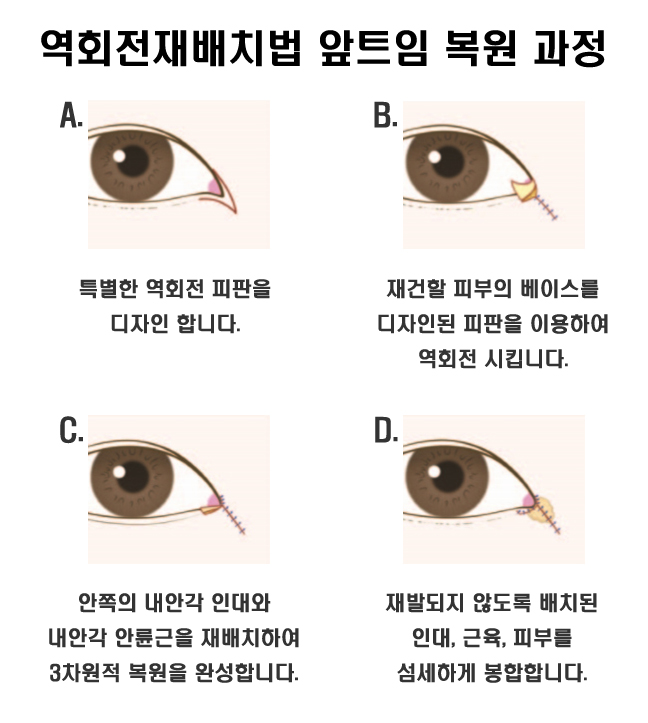
To reinforce the tissue that forms the base on the back side of the reconstructed epicanthal fold, a surgical method was devised in which the skin flap at the inner corner of the eye is lifted and rotated in reverse. This #reverse_rotation_flap_repositioning_method provides a strong base for the reconstructed epicanthal fold and helps prevent the outer skin of the reconstructed fold from reopening, thereby lowering the recurrence rate.
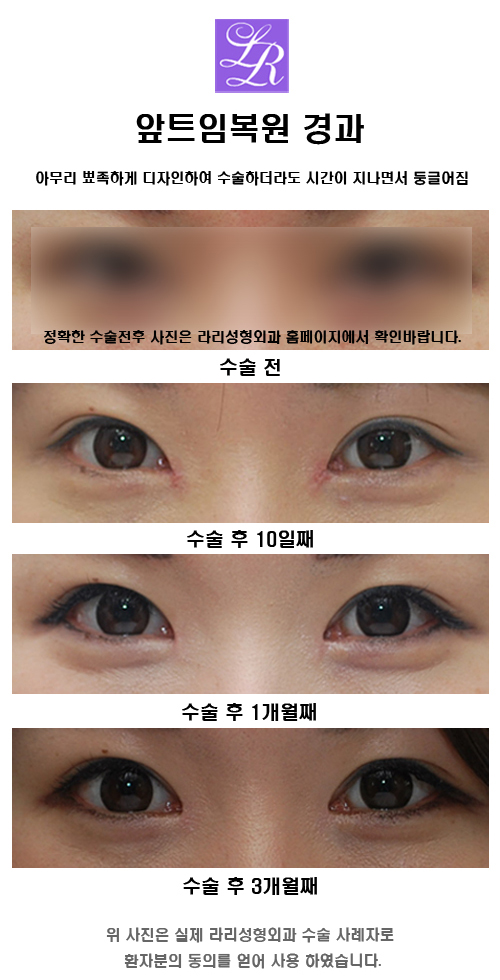
Whichever method is used, the surgery is performed under the broad principle of bringing in lacking skin from the surrounding area. Whether tissue is pulled down from above the inner eye incision or skin is pulled up from below, once it is sutured, the tissues are eventually drawn together and the epicanthal fold closes. No matter how sharply the design is made, over time the restored shape tends to become rounder because of skin tension.
Therefore, even with the most advanced medial epicanthoplasty revision technique, if there is not enough excess skin, the reconstructed tissue may reopen and a new scar may form. So the most important factor for success in medial epicanthoplasty revision is whether there is enough skin laxity.

In conclusion, there is no method or plastic surgery clinic that is 100% superior. You should avoid plastic surgery communities or apps where non-experts are active, and instead visit in person and consult directly with a board-certified plastic surgeon. That is still the path with the lowest chance of failure.