On entering~~~
People who come for consultations because they are considering facial contouring surgery have a variety of reasons and motivations, and some may also have vague expectations about how their appearance will change after surgery.
Of course, I think those who have visited me for an in-person consultation will remember to some extent,
but when I counsel patients about facial contouring surgery, the three points I emphasize most are the following.
First, even if you have facial contouring surgery, your face shape will not change within 2 weeks to 1 month after surgery.
Second, facial contours are not determined by the facial bones alone. The condition of the soft tissue covering the facial bones (the facial muscles, fat, and other soft tissues) is also extremely important, so even if the bones are reduced as much as possible, the change may be minimal if there is a lot of soft tissue on the face.
Third, if you decide to have facial contouring surgery in order to make the two sides of the face symmetrical, you may regret it greatly after surgery.
When I begin a consultation, I first ask the person why they are considering facial contouring surgery (their chief complaints).
If improving asymmetry is the top priority, I explain clearly that it is impossible to make the face perfectly symmetrical, so they may be disappointed.
Then,
I will explain why someone might be disappointed if they expect facial contouring surgery to dramatically improve asymmetry.
If you observe people’s faces closely, everyone has slightly different face shapes on the left and right sides.
If you look carefully, it is no exaggeration to say that there is no one whose face is perfectly symmetrical on both sides.
First, it is necessary to understand what causes these differences in face shape.
The reason for differences in facial contour is largely because the conditions of the facial bones and the soft tissue of the face differ between the two sides.
Looking at soft tissue differences, one can consider cases where the volume of the masseter muscles used for chewing or the amount of fat tissue in the face differs from side to side.
The difference in soft tissue can be expected to be reduced by adjusting the amount of injection or the amount of fat suctioned, taking the difference between both sides into account in procedures such as Botox injections that reduce muscle volume or surgeries such as facial liposuction.
If the conditions of the facial bones differ on both sides, very complex variables must be considered.
When the bone conditions of the face are analyzed in detail, there are differences in the occlusal plane of the teeth, the position of the temporomandibular joint, and even the height of the orbital bones surrounding the eyes.
However, variables such as the position of the temporomandibular joint mentioned above, the difference in height of the orbital bones surrounding the eyes, and the position of the occlusal plane from a three-dimensional perspective are variables that cannot be changed through any surgery.
The reason is that part of the skull that forms the temporomandibular joint protects the brain and is connected to the base of the skull, and the orbital bones are the facial bones that protect the eyes, so it is almost impossible to move their height.
Also, even with the occlusal plane from a three-dimensional perspective, it is not realistic to expect the overall arch formed by the arrangement of the teeth to be made perfectly symmetrical.
Therefore, even with double-jaw surgery, I believe the most realistic and accurate judgment is to think that facial asymmetry cannot be dramatically corrected.
Since I think the content explained above may be difficult to understand, I will explain it using an actual case.
This is the postoperative CT scan of a person I performed contouring surgery on.

The postoperative recovery followed the usual course after contouring surgery, and the patient had a mild, agreeable personality, but after quietly struggling with concerns on their own, they carefully brought up their worries to me.
Looking at the postoperative CT, they were very worried that the surgery seemed to have turned out asymmetrical......ㅠㅠㅠ
At a glance, it does not seem unreasonable at all to worry that the facial bones were operated on asymmetrically^^
Because the inquiry came through chat, I gave a brief explanation, and they understood well and replied that hearing the explanation made them feel relieved.
If they had come in person for a follow-up and asked, I would have explained it while looking at the CT from various angles directly, but there was a limit to how much I could explain through chat.
After wondering how I could explain it more clearly~~~ I thought that writing a detailed post would be the best way, so I prepared it as reference material for this post.
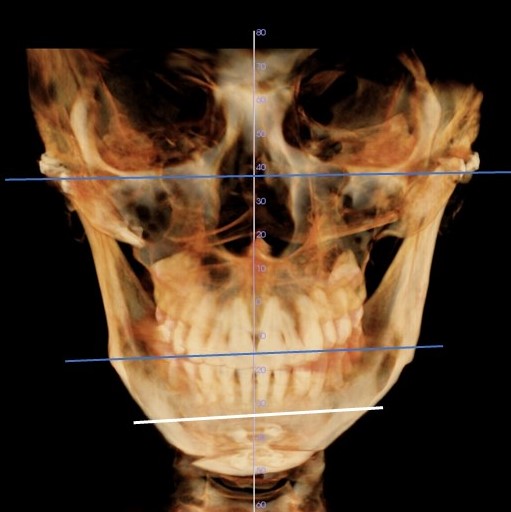
First, if you look at the distance from the center line to the temporomandibular joint, marked horizontally at the top on the CT, the distance to the left temporomandibular joint is wider than on the patient’s right side (left side in the photo).
Based on the lower edge of the orbital bone, you can observe that the right orbital bone is slightly lower than the left.
When looking at the middle horizontal line of the occlusal plane and
the lowest horizontal line (connecting the openings through which the nerve enters inside the jawbone), the right side is slightly tilted downward.
In conclusion, the length of the jawbone on the right side is a type that extends slightly farther downward, and the degree to which the jawbone spreads outward is wider on the left side than on the right.
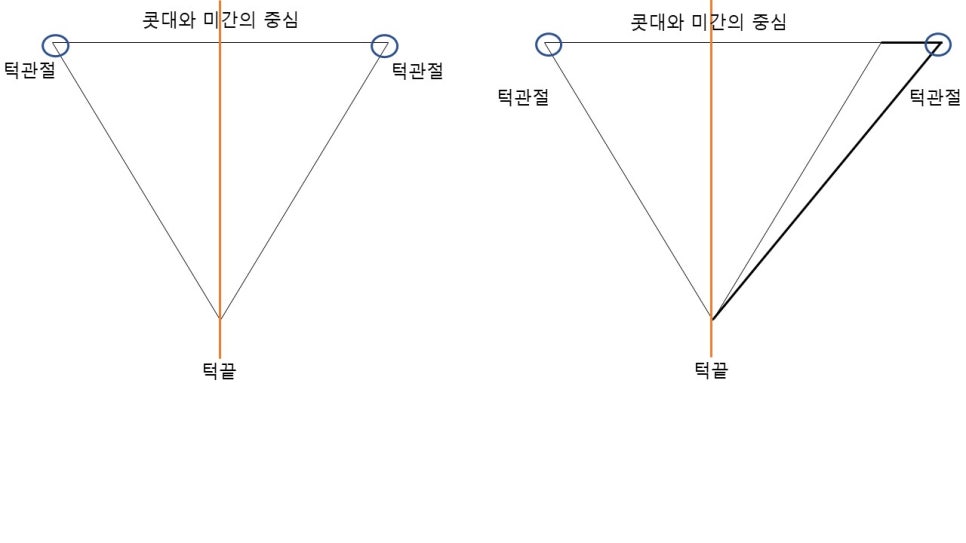
Therefore, as shown in the triangular diagram below, when we think of the positions of the temporomandibular joints and the center of the chin as the three vertices, it is not possible to create a perfect isosceles triangle.
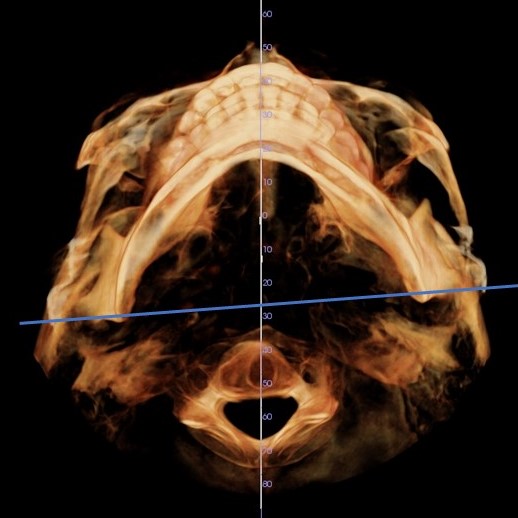
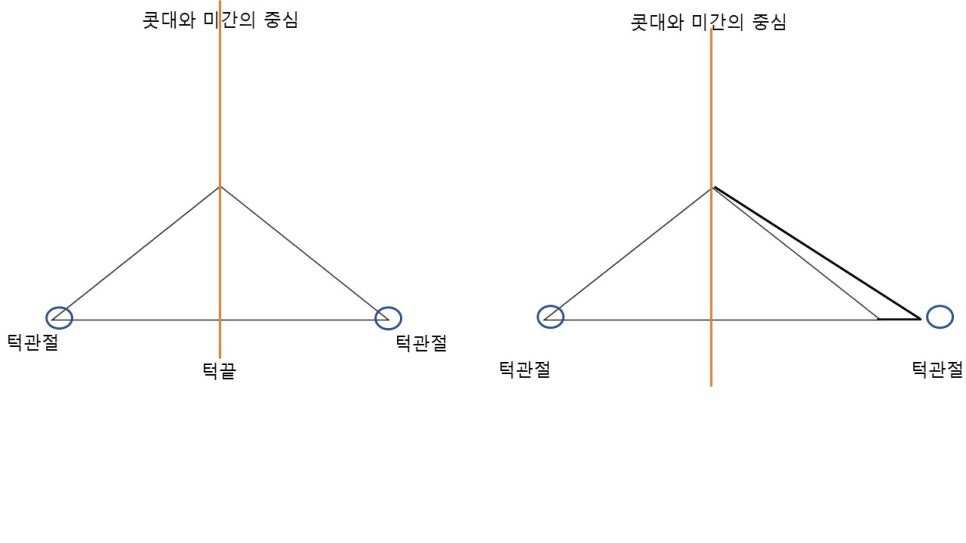
If you look at the arch shape of the occlusal plane with the head tilted back, you can see differences between the left and right sides.
In such cases, because the position of the temporomandibular joint cannot be moved, it is not possible to create an isosceles triangle in which the degree of spread from the center line is the same when viewed from the front,
and the arch of the jawbone viewed from below with the head tilted back cannot be made symmetrical either.
As I explained at the beginning,
although the degree varies, everyone has slightly different positions of the left and right temporomandibular joints, and the height of the nerve line and the occlusal plane also differ slightly.
When performing this type of surgery, the most important point the surgeon must consider is which areas should receive the most careful attention in order to reduce the degree of difference.
In this patient’s case, what I considered important and focused on during surgery was,
I tried to reduce the lower edge of the right lower jawbone, which appears longer downward, more extensively (closer to the nerve line),
and I focused on reducing the cortical bone of the body of the left lower jawbone, which is more widely spread outward, as much as possible.
Of course, during the consultation, we agreed not to touch the angle area of the lower jaw and to leave it as it was, so only the angle area was preserved intact^^
Considering the various conditions, I believe the surgery proceeded well in the direction I had carefully considered, and I sincerely thank the patient for trusting me after much thought and entrusting the surgery to me. I truly hope for a good result.