Many people considering cheekbone reduction hope for or expect one thing: “a narrower face in the frontal view.”
To achieve the maximum effect of a reduced facial width from the front, the area where the zygomatic arch is widest must ultimately move the most.
However, many people find that after cheekbone reduction surgery, the facial width does not decrease effectively, and they often end up considering revision surgery. In fact, satisfaction is often high after revision surgery.
For this reason, interest in posterior zygoma or back zygoma reduction has increased, and many people only come to know about it later, after initially researching and deciding on cheekbone surgery.
Many of the people who visit my clinic are also considering cheekbone revision surgery because they did not experience meaningful changes after surgery elsewhere, and they often request consultations about the posterior zygoma, or back zygoma.
However, when I listen to the various stories from people who come for consultations...
I realize that many people have a very incorrect understanding of posterior zygoma reduction.
Therefore,
In this post, I will explain based on 3D CT scans that I analyzed from people who came to consult with me directly.
-
When did the terms “posterior zygoma” and “back zygoma” begin to be used, by whom, and how?
-
What 기준 points can be used on postoperative CT to determine the reduction effect in the posterior zygoma area?
-
What are the problems with places that distort and promote posterior zygoma reduction?
-
What is the correct understanding of temple reduction, and what are the problems with places that imitate and promote a procedure called “temple reduction”?
Overall Understanding of Cheekbone Reduction Surgery
The cheekbone is one part of the facial bones responsible for the contours of the middle part of the face.
Anatomically, the cheekbone consists of the body and the arch.
The body of the cheekbone, located in the front portion of the face, is responsible for the contour of the area connecting below the eye to the outer lower area of the eye corner, while the zygomatic arch forms the bulging contour below the temple and plays a role in determining the width of the middle face.
If we look closely at the structure of the zygomatic arch, which determines facial width and forms the contour of the side cheekbone, it flares outward toward the back.
In other words, the zygomatic arch becomes wider as it goes toward the rear!!!
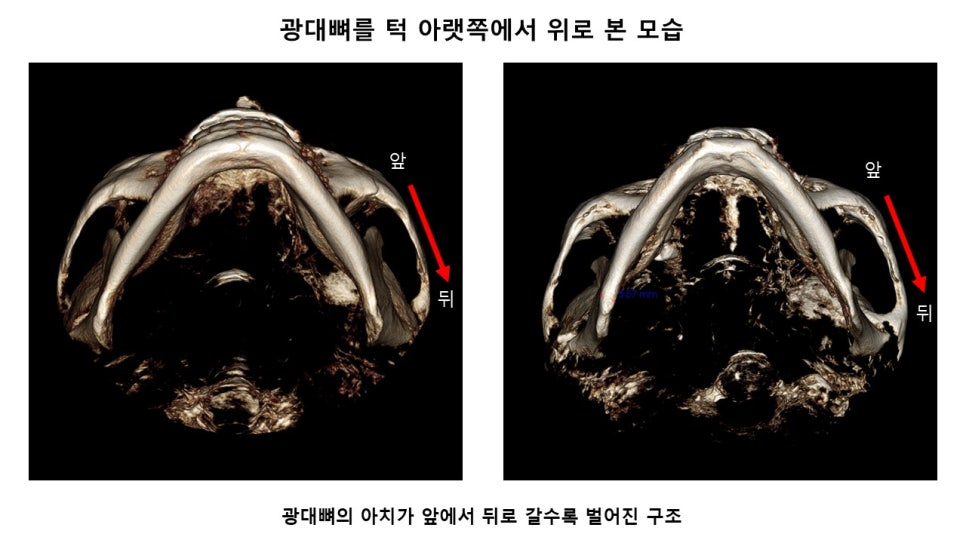
Therefore, in order for cheekbone reduction surgery to narrow the facial width and create a more three-dimensional face, surgery is needed in a direction that maintains appropriate volume in the front cheekbone and 45-degree cheekbone area while moving the widening zygomatic arch inward as much as possible.
The Origin and History of the Terms “Posterior Zygoma” and “Back Zygoma”
The terms “posterior zygoma” or “back zygoma” were not first used by me, and they were certainly not terms that had long been used in the plastic surgery field.
Then who was the first to use and spread the terms “posterior zygoma” and “back zygoma”?
This goes back 11 years from now, to 2014.
There was a medical student who came to consult with me seven times and eventually underwent surgery.
I introduced the story about him on my blog long ago (https://blog.naver.com/cantata147/220384841877)
After receiving surgery from me, he posted various things on the plastic surgery community where he was active, and the most memorable among them was the statement that
“Director Jeong Jae-young of Lavian Plastic Surgery has identified that the cheekbone is cut at the very rear-most portion.”
After that student had surgery with me, many people came to me for consultations and asked using the term “rear-most osteotomy”...
I heard the term “rear-most osteotomy” for the first time at that time.
Although I had given many presentations on cheekbone reduction surgery at plastic surgery academic conferences, written papers, and even demonstrated surgery at international academic meetings, I had not thought that there was a major distinction in the osteotomy location in the posterior portion of the cheekbone arch.
From that time on, among the general public interested in cheekbone reduction surgery, the expression and concept of “back zygoma” or “posterior zygoma” began to circulate.
Reference Point for Determining the Degree of Cheekbone Reduction on 3D CT Before and After Surgery
When cheekbone reduction surgery is performed, an objective reference point is absolutely necessary in order to assess the degree of change in the posterior zygoma and side cheekbone on pre- and postoperative 3D CT.
I will explain what should be chosen as the reference point.
In cheekbone reduction surgery, the area that cannot be changed must serve as the 기준 for determining and measuring the difference before and after surgery.
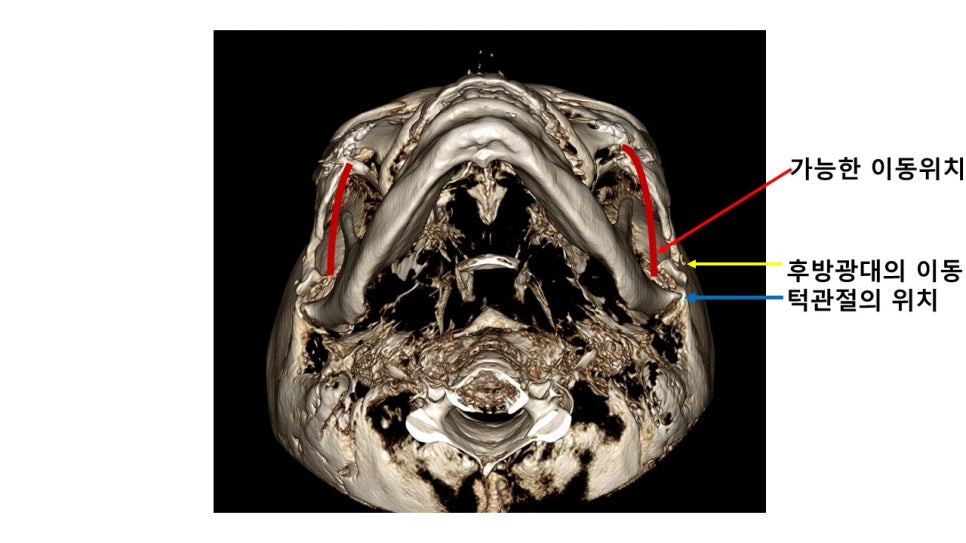
The area that should not be touched or affected during surgery is the temporomandibular joint.
The location of the temporomandibular joint is the area marked with a yellow circle in the CT below.
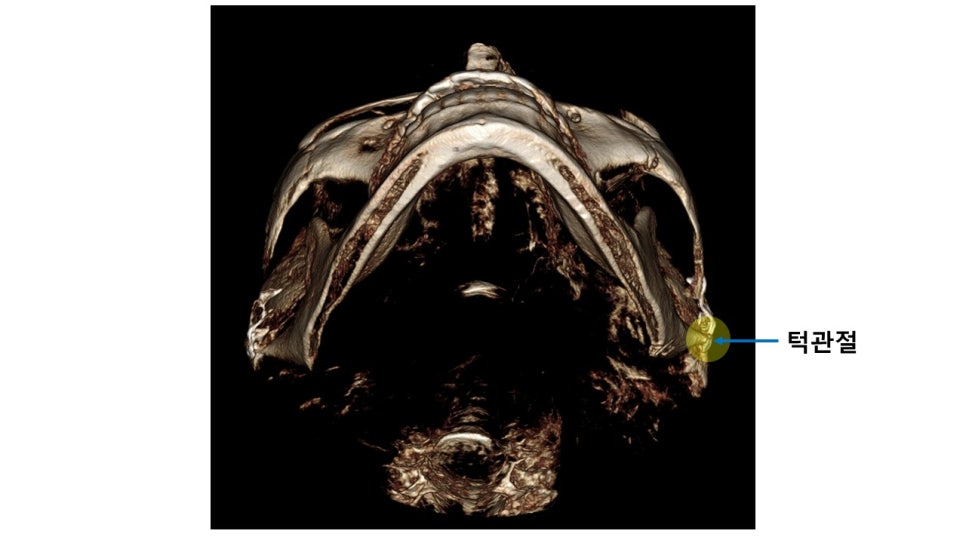
Location of the temporomandibular joint on postoperative CT after cheekbone surgery
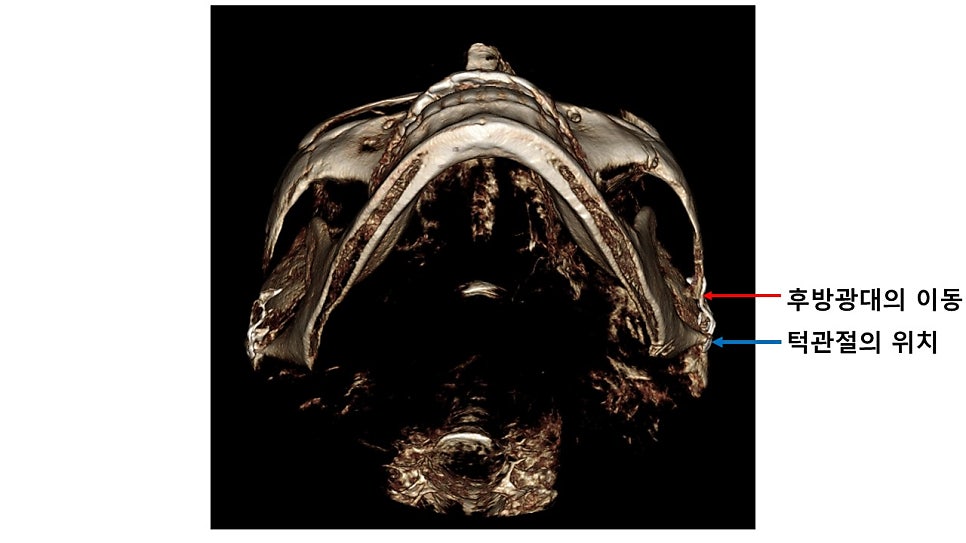
The CT below shows the location of the temporomandibular joint and the amount of movement of the side cheekbone, including the posterior zygoma.
It can be seen that it has moved far inward from the position of the temporomandibular joint.
Problems With Places That Misrepresent Posterior Zygoma Reduction
The number of people who come to me for revision surgery or even a third surgery after having surgery at a place that advertises that it effectively reduces the posterior zygoma (and also performs temple reduction...) has been increasing quite a bit.
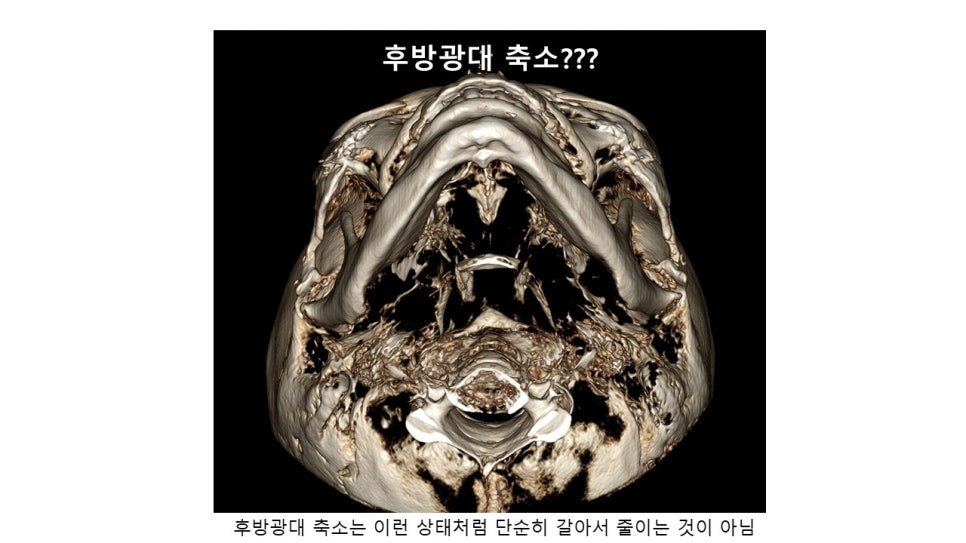
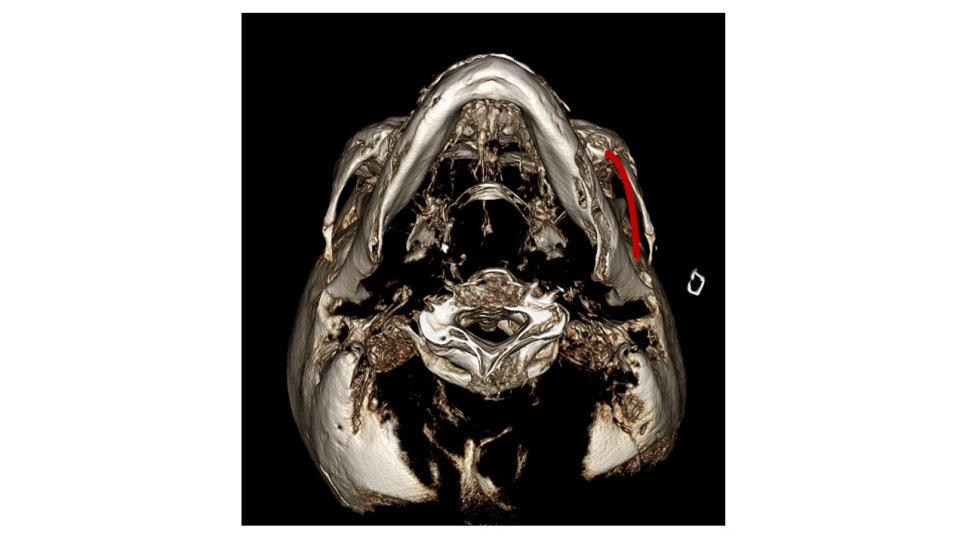
Let us look at a 3D CT of someone who had surgery at such a place and consider the problems.
If you look at the CT below, you can see that they simply shaved down the area just in front of the temporomandibular joint.
When surgery is performed this way, not only is the reduction effect on the side cheekbone including the posterior zygoma minimal, but the bone in the posterior portion of the zygomatic arch that forms the temporomandibular joint and posterior zygoma is also shaved away, leaving it in a state that is almost impossible to fixate.
Therefore, this effectively eliminates the possibility of further reducing the posterior zygoma or side cheekbone...


Correct Understanding of Temple Reduction
I often hear from people who come for consultations that some places are misrepresenting temple reduction as a procedure with definite effects.
However, I think that is highly irresponsible, either a mistaken belief due to lack of experience or an exaggeration for commercial purposes.
I have been performing temple reduction for more than 20 years already, and even after I first presented that I would perform temple reduction together with cheekbone reduction surgery, no one mentioned temple reduction for another 10 years.
The reason I had no choice but to perform temple reduction was that when the side cheekbone and posterior zygoma are reduced effectively, the temple area above the posterior zygoma may appear relatively bulged as the swelling subsides after surgery.
This temple reduction surgery directly reduces the temporalis muscle and fat pad that create the volume in the temple area.
The procedure itself is very safe and has been validated over a long period of time.
However, temple reduction surgery alone often makes it difficult to expect a major surgical effect, and even if the temporalis muscle is cut, the remaining temporalis muscle may sometimes thicken the muscle fibers to compensate for the reduced and resected muscle.
Therefore, it is best not to expect too much from temple reduction.
In this post, I explained based on actual CT images from real cases in order to help clarify the misconceptions and correct understanding regarding posterior zygoma and back zygoma reduction.