The purpose of cheekbone reduction surgery is broadly divided into two goals.
First, to make the face narrower and softer by reducing the lateral cheekbones, which determine the width of the area below the temples and the middle part of the face.
Second, to gently refine the contour of the cheekbones that protrude at a 45-degree angle, softening the prominent cheekbone shape seen from the front and from a 45-degree angle.
With the lateral cheekbone reduction effect in this type of cheekbone reduction surgery, one can expect the facial width to decrease by up to about 15 mm on one side.
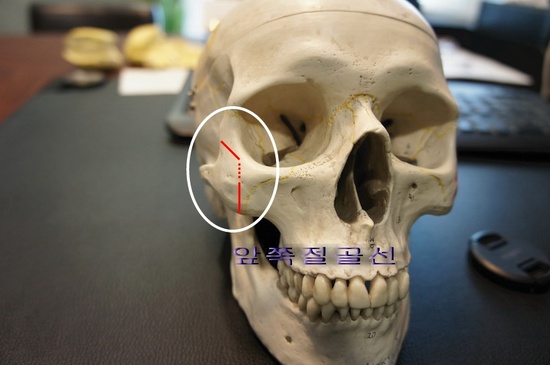
As shown in the figure above, if the lateral cheekbone, which has spread outward, is moved inward based on the anterior osteotomy line and fixed in the correct position, a consistent and predictable result can be expected.
However, depending on the surgical method, if the bone is not cut at the correct area or the fixation is not done properly, the following results may occur.
 First, if the anterior osteotomy is not done accurately, the postoperative result will be little different from the preoperative state.
First, if the anterior osteotomy is not done accurately, the postoperative result will be little different from the preoperative state.
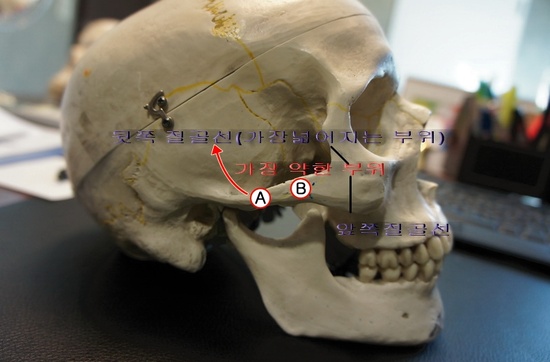
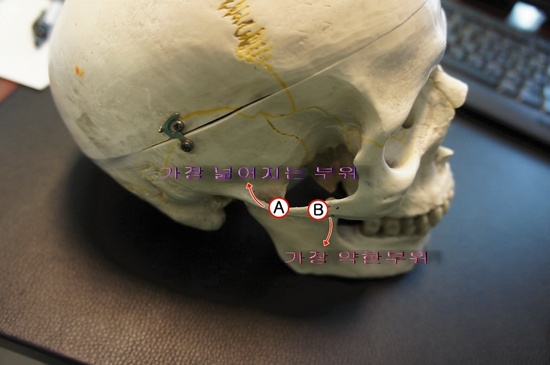
Second, since the widest part of the lateral cheekbone contour is the A area, if the posterior osteotomy line is not identified accurately and is pressed by hand imprecisely, it can lead to the unfortunate result of breaking the B area, which is the weakest part of the cheekbone.
In such cases, the face may appear to step backward, and the two sides may show a severe difference; in some cases, revision surgery may become almost impossible.
Third, if the anterior and posterior parts are cut but not fixed, the cheekbone segment between the osteotomies may sag downward, causing nonunion and creating a high risk of a result that makes the face look drooped.
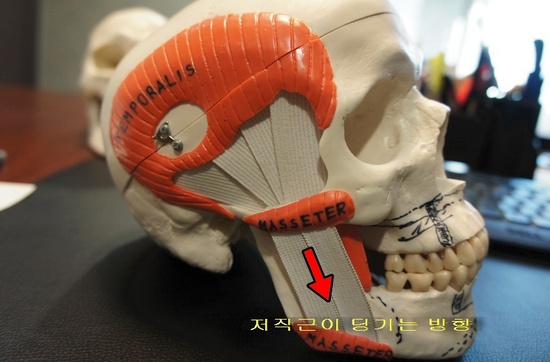 If the anterior and posterior osteotomy lines of the cheekbone are not properly cut, the postoperative result will only be little different from the preoperative state. However, if the parts where the masseter muscle is attached (the area marked MASSETER) are cut at the front and back but are not fixed in the correct position, the bone will sag downward in the direction pulled by the masseter muscle.
If the anterior and posterior osteotomy lines of the cheekbone are not properly cut, the postoperative result will only be little different from the preoperative state. However, if the parts where the masseter muscle is attached (the area marked MASSETER) are cut at the front and back but are not fixed in the correct position, the bone will sag downward in the direction pulled by the masseter muscle.
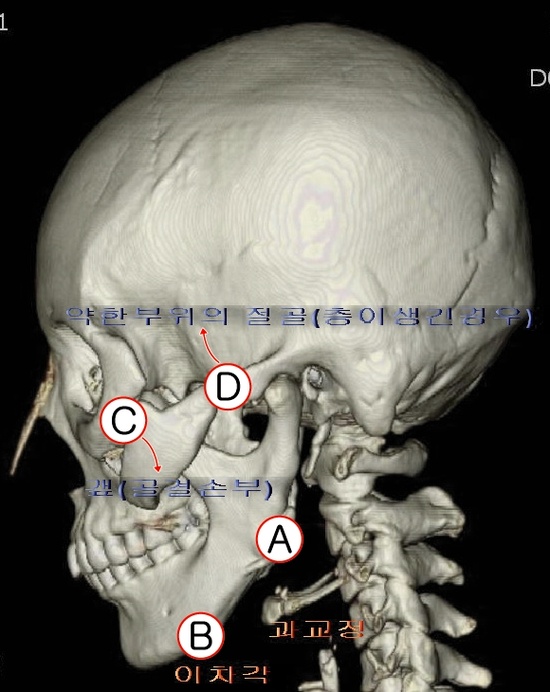
Below is an actual three-dimensional CT scan of a person with the problems described above.
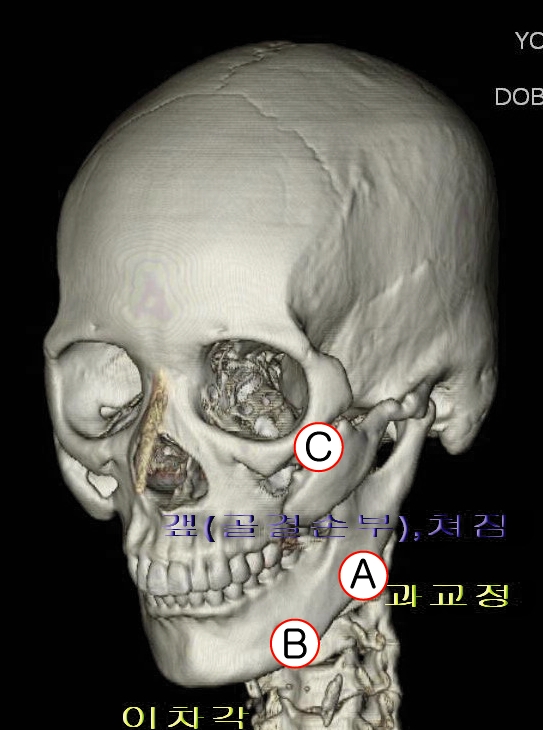
This shows the bone defect area (C) caused by cutting and not fixing the front part of the cheekbone, and the bone in a sagged downward position.
In jaw angle surgery as well, the posterior angle area shows excessive overcorrection (A), and an uneven secondary angle (B) has formed at the front.