Recently, after zygomatic reduction surgery, many people have noticed that the osteotomy site has opened up and, feeling anxious, have come to the author to consult about revision surgery.
I think that trying to make zygomatic reduction surgery easy and simple using various methods may be one reason why a number of problems arise.
To begin with the conclusion, if a certain part of the zygomatic bone is fixed and does not move, then the gap at the osteotomy site that appears after zygomatic surgery itself is not a major problem.
Even so, after visiting several plastic surgery clinics for consultations, some people are told that even a small 2~3 mm gap is a serious problem. Because of that anxiety, they cannot even lie down comfortably to sleep and come to see the author.
Of course, in zygomatic reduction surgery, if it were possible to perform the surgery in a way that does not leave any gap at the osteotomy site, that would be the most ideal.
If the continuity of the zygomatic area, which determines the contour of the central face, is maintained while effectively reducing the lateral cheekbones, one can expect the facial contour to change into a smaller yet more three-dimensional shape.
Let us consider why the osteotomy site of the zygomatic bone opens up and creates a gap, and what methods of surgery can maintain the continuity of the zygomatic bone after surgery so that it remains seamless.
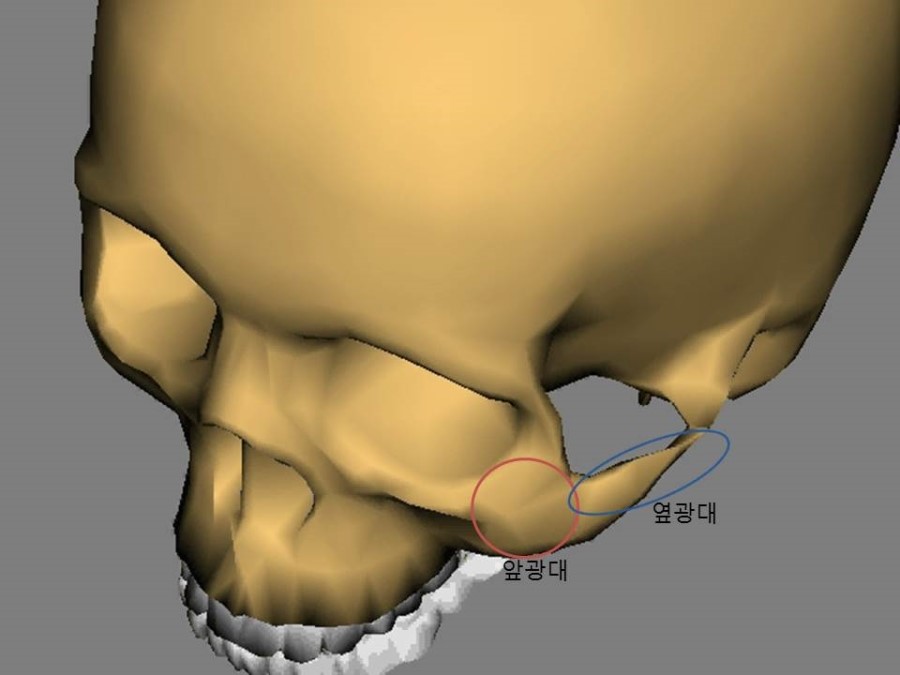
The zygomatic bone is medically called the Zygomatic Complex or Malar Complex. If we look closely at the meaning of “complex,” the name comes from the fact that it is composed of the Zygomatic Body or Malar Body and the Zygomatic Arch or Malar Arch.
The author believes that the most important thing in surgery that changes the contour of this zygomatic complex is to operate with continuity and harmony of the zygomatic complex in mind.
If we look at each part of the zygomatic complex separately, the Zygomatic Body or Malar Body is responsible for the contour of the front cheekbone that protrudes forward, while the Zygomatic Arch or Malar Arch is responsible for the contour of the lateral cheekbone that bulges below the temples.
Recently, the expression “45-degree cheekbone reduction” is often used, but from the author’s perspective, the term “45-degree cheekbone reduction” is a name created as a promotional device.
Of course, the area connecting the front cheekbone to the lateral cheekbone can be casually referred to as the 45-degree cheekbone, but if one understands the surgical methods and the changes below, it becomes clear how pretentious the expression “45-degree cheekbone reduction” is.
If you understand the surgery that reduces the cheekbone area above correctly, there are the following methods.
1.
- A method of cutting out the body of the cheekbone and fixing it
2.
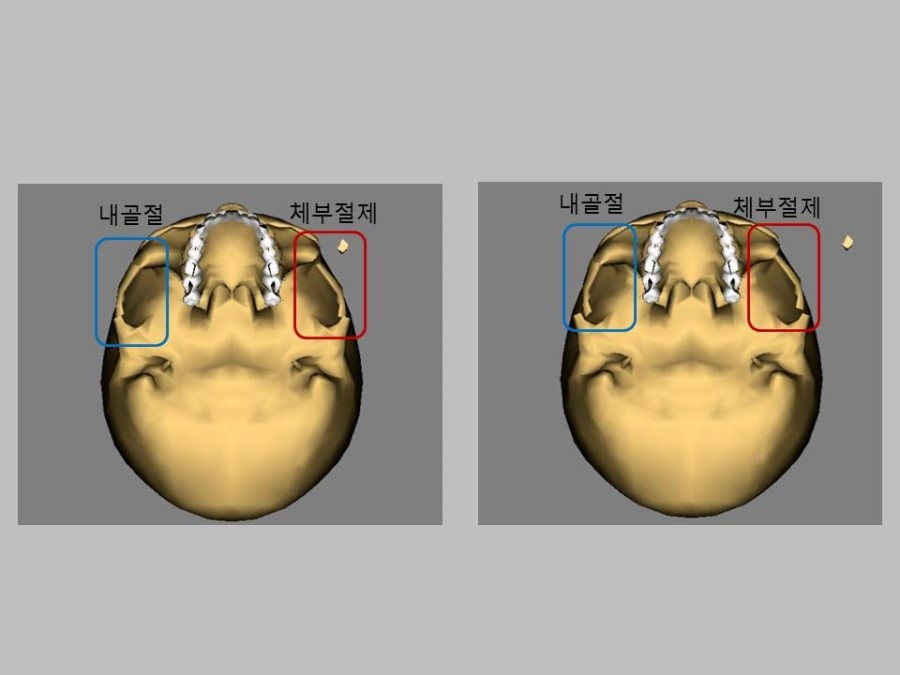
2. A method of osteotomizing an appropriate area connecting the body of the cheekbone to the lateral cheekbone and bringing it inward
The author believes that if fixation is not performed in zygomatic reduction surgery, it is not a proper surgical method, and because I have seen too many cases of damage, I will not separately discuss non-fixation cheekbone surgery.

The method most commonly used is to cut out the body of the cheekbone and fix it in place. However, in my case, I use the method of cutting and fixing the front cheekbone only when the front cheekbone is very wide and its width must be reduced significantly. The reason is that the continuity of the cheekbone may be somewhat disrupted.
 Case 1
Case 1
 Case 2
Case 2
 .
Case 3
.
Case 3
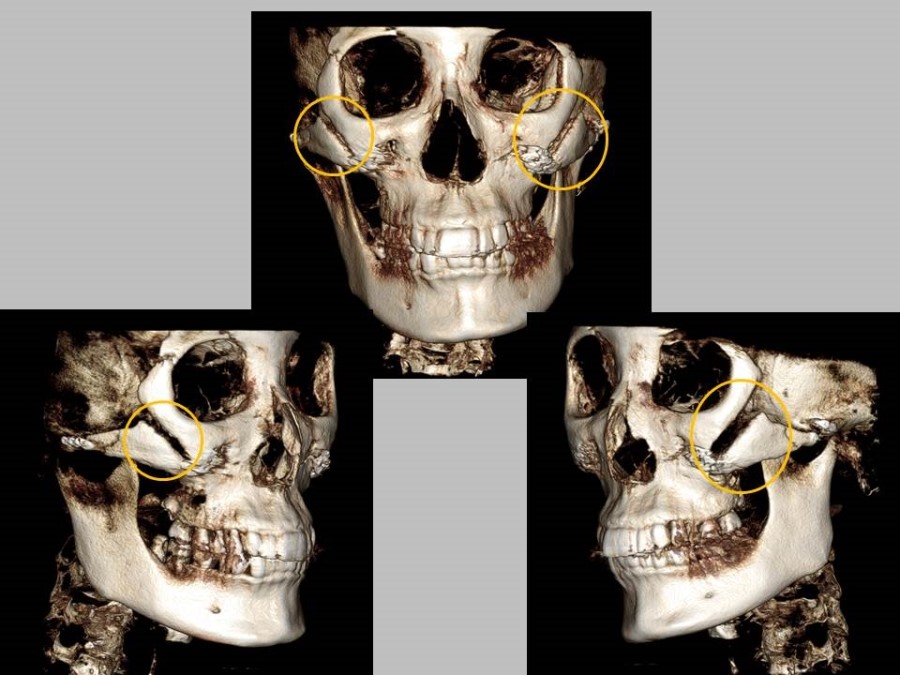
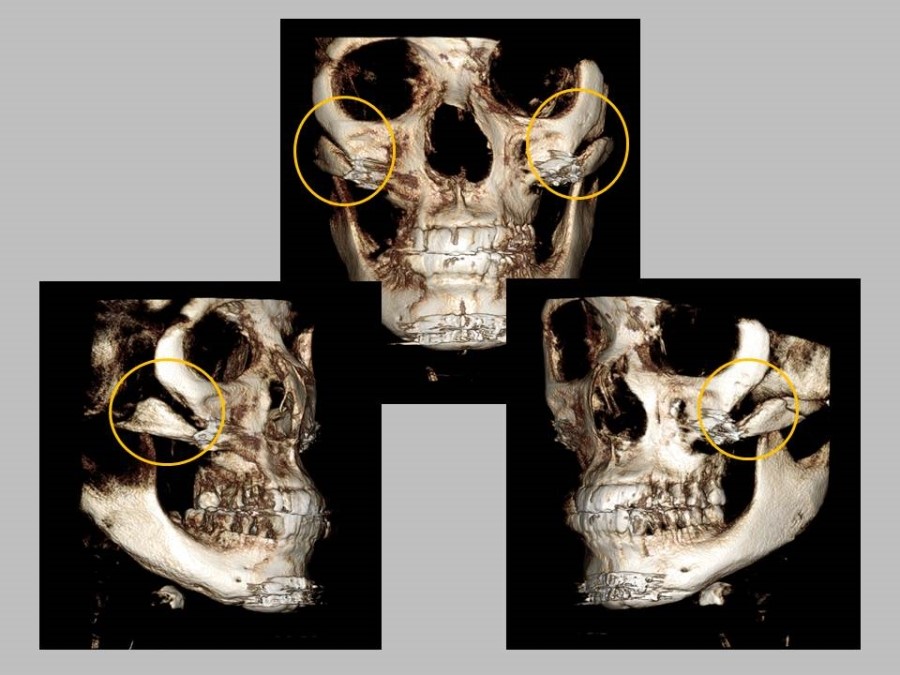
The cases above are examples of people who came to consult the author about revision surgery because, in order to reduce the 45-degree cheekbone, the body of the cheekbone was removed and the lower part was fixed, leaving a gap in the cheekbone area.
Of course, even though large gaps like this do not occur often simply because the body of the cheekbone is cut out, the continuity connecting the front cheekbone to the lateral cheekbone can easily be disrupted, and there are many cases in which it is difficult to expect a proper reduction effect on the lateral cheekbone.
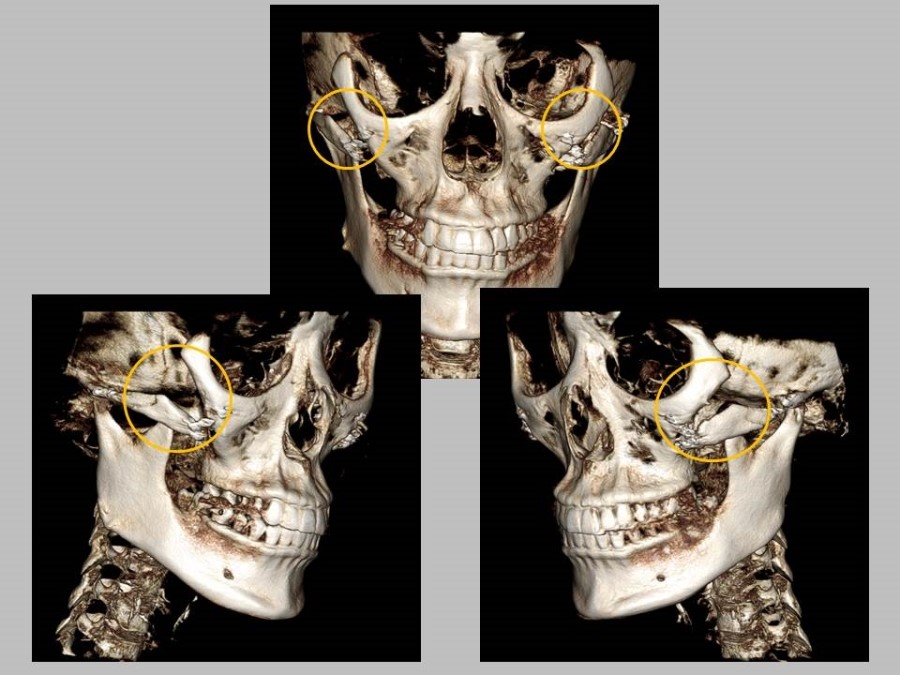
The 3D CT images below are cases in which zygomatic reduction surgery was performed using an internal osteotomy.
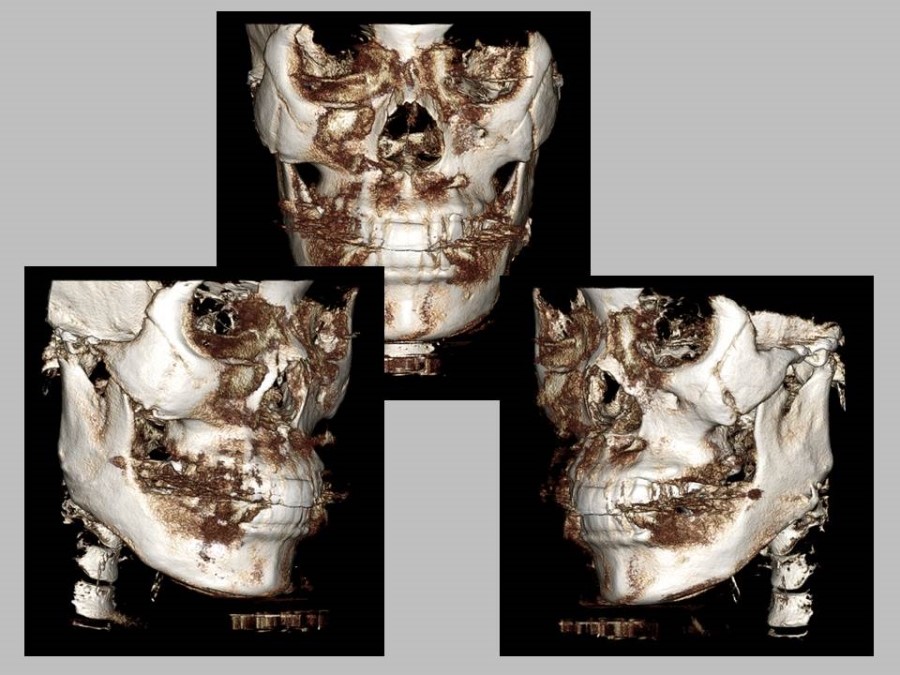
In conclusion, even if the osteotomy site of the cheekbone is open, there is no need to worry too much if it is fixed. However, in most cases, if the reduction effect on the lateral cheekbone, which reduces the width of the face, is insufficient and revision surgery is being considered, I think there can be sufficient reason to consider a secondary procedure.