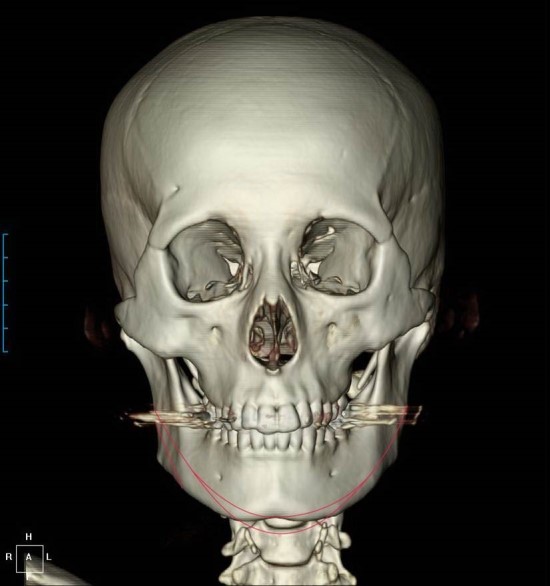
In a typical face shape, when the face is viewed from the front, the widest area is the lateral zygoma area.
In such cases, it can be said that the width above and below is determined to some extent, starting from the point where the lateral zygoma is widest, with the temple area above and the angular area of the lower jaw below.
Therefore, in a typical face shape, the width of the face is largely determined at the area behind the lateral zygoma, where the widest part of the lateral zygoma becomes the highest pole of the tent (Bizygomatic Distance), and is secondarily determined at the temple area, which is a somewhat lower pole position (Bitemporal Distance), and the angular area of the lower jaw (Bigonial Distance).
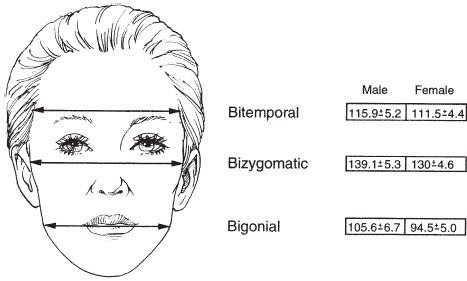
As explained above, if you average the statistics, the lateral zygoma is the widest part of the face, followed by the width of the temple area, and third is the angular area of the lower jaw.
However, there are also face shapes in which the temples are the widest part and the face becomes narrower toward the lower part.
In such cases, performing lateral zygoma reduction together with temporalis reduction has the effect of reducing the width of the face, and it may be a case with a very high level of satisfaction after surgery.
If only zygoma reduction is performed even though the temples are wide, the temple area above the zygoma may appear more protruded, creating an hourglass-like face shape.
Temporalis reduction can be said to be a surgical method that is unfamiliar to most people.
For that reason, many people have asked me about temporalis reduction while also expressing several uneasy concerns.
First, is temporalis reduction not an extremely risky surgery?
Second, some people say they have heard elsewhere that because their skull is large, the temples cannot be reduced.
Third, to reduce the temples, the skull bone would have to be reduced, but is that possible?
The reason there has not been a common awareness of temporalis reduction may be that, until now, zygoma reduction surgery has not produced results capable of effectively reducing the lateral zygoma. However, I have long been working on temporalis reduction because I had been concerned that, when the width of the lateral zygoma is greatly reduced, the temple area above it may appear relatively more protruded, and I reached the conclusion a long time ago that sufficiently safe and satisfying results can be expected with a simple procedure.
It is a method that has been verified over a period of about 10 years, and I think it is fair to understand that there have been no cases of side effects after temporalis reduction.