When I decided to open a practice in a fiercely competitive area and set up a survival strategy, I mainly thought about quality competition and differentiation among the ways to compete: competing on price, competing on quality, or differentiating our business in areas other than price and quality. But if I wanted to become one and only through differentiation, I felt I needed to ask whether the direction of that differentiation was actually something the market wanted. To give an extreme example, an omakase dental clinic that treats any tooth however it wants regardless of the patient’s wishes might have a uniquely differentiated feature, but very few consumers would actually want that.
However, there is no need to insist on just one of the three methods. For example, even if I chose quality competition as my main strategy, there could still be specific treatments where I compete on price. Depending on who I regard as the competitor, there may be cases where fee competition is necessary. In practice, I aim for premium pricing, but I do not think every treatment has to be priced at the premium level. Rather, I believe it is important to find an appropriate price that maximizes consumer benefit and my management goals at a level the market can accept.

I try to charge accordingly for procedures that require a dentist’s expertise and long treatment time. A representative example is resin restoration. Another is powder scaling, which I perform myself and which also has a relatively high fee. In both cases, because I must directly invest my own labor, I cannot provide the service at a low fee. To make treatment cheaper, the doctor’s procedure time must necessarily be shorter. In Gangnam, being able to offer implants at a low fee is possible because everything except the “surgery itself” is illegally delegated to people who are not medical professionals. When outcomes are poor, it can even be the practice managers, and at times security staff, who handle the cleanup instead of the doctor.
However, for treatments such as drug administration, where most of the effect is determined by the drug itself, our clinic has a hard time maintaining premium fees for things like bruxism Botox. In such cases, fee competition is unavoidable, and instead we need to work to win back demand that has been taken by dermatology and aesthetic clinics. In other words, my competitor in the bruxism Botox field is the aesthetic clinic. That means the pricing benchmark also has to be set against dermatology. So if we are mainly competing on quality in resin restorations, then more price-competition elements enter into bruxism Botox. It would not be wrong to say that, through real-world experience, we are finding the balance point by seeing how price elasticity responds along the supply-demand curve.
Dentists oddly tend to set lower fees for procedures that require more of their own expertise and labor than for treatments that do not. Perhaps that is due to defeatism after becoming accustomed to the distorted insurance fee structure, but more likely it is simply because they have never once thought seriously about this strange pricing structure. For example, Botox seems expensive to many dentists because it is not a treatment they perform every day and therefore feels rare. But from the patient’s perspective, Botox is a common product with many substitutes. By contrast, treatments like resin restoration require the dentist to pour in their full expertise and time, and they are a monopolistic medical service that cannot be found in any department outside dentistry, yet most clinics price them very low. Because of that, the desire to develop gets blocked, and the cost that is put in gets squeezed even harder.
Instead, dentists are extremely sensitive only to “implant fees.” That is probably because implants were the highest-priced single procedure item (in the past tense). But I think the big mistake was delegating the competition not to the doctor’s own expertise or to the essence of the treatment as “the prosthetic transplant surgery that replaces a lost tooth,” but to the fame of the implant company, thereby turning implant treatment itself into something more like “selling a mass-produced product” than a medical act. This competitive flow has become so large that no individual can easily go against it, and implant prices have collapsed to a point that is no longer recoverable. In a normal private clinic structure where the head doctor handles everything from A to Z before and after the procedure, it is impossible to offer implants at such destructive prices, so it is difficult for a small clinic to compete on implant fees.
That is why I thought it would be more rational to raise fees in areas where the principal doctor’s expertise is high and where labor input and stress are greater. So I began reorganizing treatment prices based on the fees of procedures that serve as competition/comparison benchmarks for each treatment. For example, the comparison for Class II resin restoration would be an inlay. Then the fee for Class II resin restoration should be set with the inlay as the benchmark. In fact, my fee for Class II resin buildup is higher than the fee for an inlay. As I said earlier, that is because my expertise, labor input, and treatment stress are greater for Class II resin buildup, and also because from the patient’s perspective, it removes much less tooth structure and the treatment is completed in just 30 minutes in a day. In a similar way, the comparison for my anterior resin treatment is always laminate veneers and crowns, not the resin prices of other clinics.
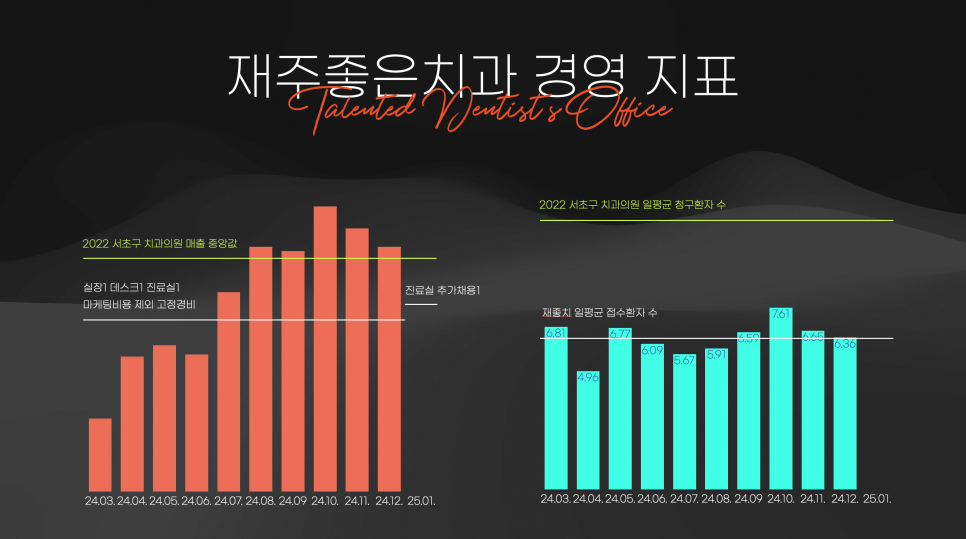
To speak with actual management numbers, I think the biggest advantage of operating with premium fees has been proven by the fact that, with about half the number of booked patients per day compared with the Seocho-gu average, I achieved gross revenue higher than the Seocho-gu median. If calculated using fixed costs excluding marketing expenses, this year’s management performance is actually quite decent. However, if I include the marketing expenses spent over the year, it is definitely true that we are in the red. And if I add loan repayment amounts and retirement reserve contributions... I should stop here because it makes me sad. Anyway, the point is that I believe raising fees in treatments other than implants and competing on quality can clearly become a survival management model for Jaejotchi Dental Clinic. If I switched to a low-fee concept, would the number of visitors increase? And if the same number of visitors came under a low-fee model, would revenue have turned out like that? In the end, a small clinic has to fight in areas where large discount-driven clinics cannot. That means rediscovering value in work that consumes the doctor’s time. There is no need to jump into the arena that the large discount clinics are risking their lives to defend.
The hardest part of opening a new clinic in the fiercely competitive old district of Gangnam is not rent, but the fact that marketing costs keep rising without limit. Money keeps going into marketing that is hard to measure, and those costs are truly enormous. That also means that, for the most part, advertisements do not have much pull. It is said that the ad spend needed to hook and bring in one patient near Gangnam Station can be as high as 300,000 to 600,000 won per person. That means if you provide treatment cheaper than that, you are operating at a loss. So they hook patients in with low prices first, then add various extra charges or recommend unnecessary treatments to increase the final payment amount. But I do not even have the budget for that kind of ad spending, and I do not intend to hook patients with price in the first place, so I felt that the efficiency of typical advertising methods was not very high. Of course, the fact that the market conditions have become so bad also played a part in my decision not to renew my contract with the marketing agency. I set a goal to cut marketing expenses even further in 2025.
After opening a new clinic in the competitive old district, I became firmly convinced that the “existing patients” possessed by an acquired practice are an enormous asset. It is a powerful weapon that lets a clinic start generating profit from the beginning. I think it is such an overwhelmingly powerful weapon that paid marketing is almost unnecessary. If there are people in Seoul preparing to open a clinic around me, I would definitely recommend acquiring an existing practice as the first option. But as more existing patients accumulate for me in the future, the number of daily patients will increase, and then the average revenue per patient will fall, so even if daily patient volume doubles, revenue will not double. Now I need to prepare for that future.
Jaejotchi Dental Clinic focuses on anterior resin treatment that preserves the transparent layer, so in that sense it is the exact opposite of Minish. In some ways, I also want it to be the opposite of Plan and Seokplant. As I said in the introduction to “Opening Preparation Note 4. Differentiation, Selection, and Focus,” one of the many diary entries I wrote during the opening process, the reason I chose a direction opposite to the current opening trend represented by large scale + discount + 365-day operation was precisely to provide resin conservative restorations and aesthetic retreatment at a high level of quality. If you adhere to the Biomimetic concept and the principles of bonding in order to maximize the quality of resin treatment, having dozens of patients per day is a disadvantage. That is because the doctor’s fatigue level is very high for each individual treatment. So I created a small boutique clinic.
However, I also know that for my plans and management performance to be recognized, higher revenue than we have now is required. I want revenue to increase, too. It is not enough just to survive in Gangnam; we need to achieve better results. If we could maintain the current average revenue per patient while increasing the number of daily patients to the average, that would be ideal. I naively think that, if that happens, junior doctors will also stop hesitating to raise the fees of treatments that provide real value. I myself gained courage from watching a senior director do the same. Having a role model definitely becomes a support through difficult times.
The opening market is clearly sinking at a rapid pace, but even so, there are small movements trying to keep the ship afloat. I hope that one day, when someone says, “That works because it’s Gangnam,” we can answer, “Then try it at Hankuk University of Foreign Studies,” and when someone says, “That works because they have existing patient referrals,” someone else can reply, “Jaejotchi can do that too.” It does not seem like that time has come yet...ㅠ Still, I am happy that, while taking all holidays off in Gangnam and opening a new clinic from scratch without evening hours, things do seem to be unfolding slowly in the way I intended when I first opened.
Above all, I hope that we all move forward by looking for reasons something can work, instead of reasons it cannot.
For now, I really need to focus on strengthening our moat in anterior resin treatment. From what I heard in the UK, local clinics there charge 500 pounds for the level of resin treatment I do (about 950,000 won at current rates) and 800 pounds for porcelain veneers (about 1.5 million won at current rates), which is relatively inexpensive by comparison. I believe Korean standards are in no way inferior to those in the UK, so I think we can charge that much as well. (The most famous APA in the U.S. charges 4,000 to 6,000 dollars for one veneer... at least 6 million won.)
Anyway, 2025 has arrived, and this year I want to hone my anterior resin skills even further while also making our clinic truly profitable.