Anterior resin build-up for dentists
I gave a lecture
On January 31,
at the invitation of iO BIo,
I gave a lecture on the theme of
"minimally invasive treatment (procedures that preserve as much tooth structure as possible)."

This lecture was attended by many people who are very familiar with clinical practice,
including directors who already run their own clinics and are treating patients,
associate doctors preparing to open their own practices,
and dental hygienists working together in dental clinics.

I was grateful that someone even left a review on their Instagram feed haha
Resin build-up
And the standard of minimally invasive care

These days, anterior resin build-up has become a fairly familiar treatment,
but when I was preparing to open my practice,
it was an area that was hardly discussed in Korea.
So I taught myself by looking at YouTube videos and Instagram accounts of dentists overseas haha
(I also wrote a practice-opening diary, which brings back memories haha)
Back then, when people thought of front-tooth treatment, laminate veneers or crowns came to mind first,
and resin was perceived relatively as a "light" treatment.
But while doing crown treatment,
every time I looked at the front teeth of especially younger patients,
I kept wondering whether we were cutting teeth too easily and too much.
So the standard I set was simple.
Let's think hard about how far we can preserve!
At the center of that standard is minimally invasive care,
and one of the secret weapons that makes it possible
is Qray, which I always use.
If you ask why I insist on Qray,
there are actually downsides too, because using Qray makes treatment take longer,
and the patient has to keep their mouth open, so it can be uncomfortable.

Even so,
the reason I use Qray is clear.
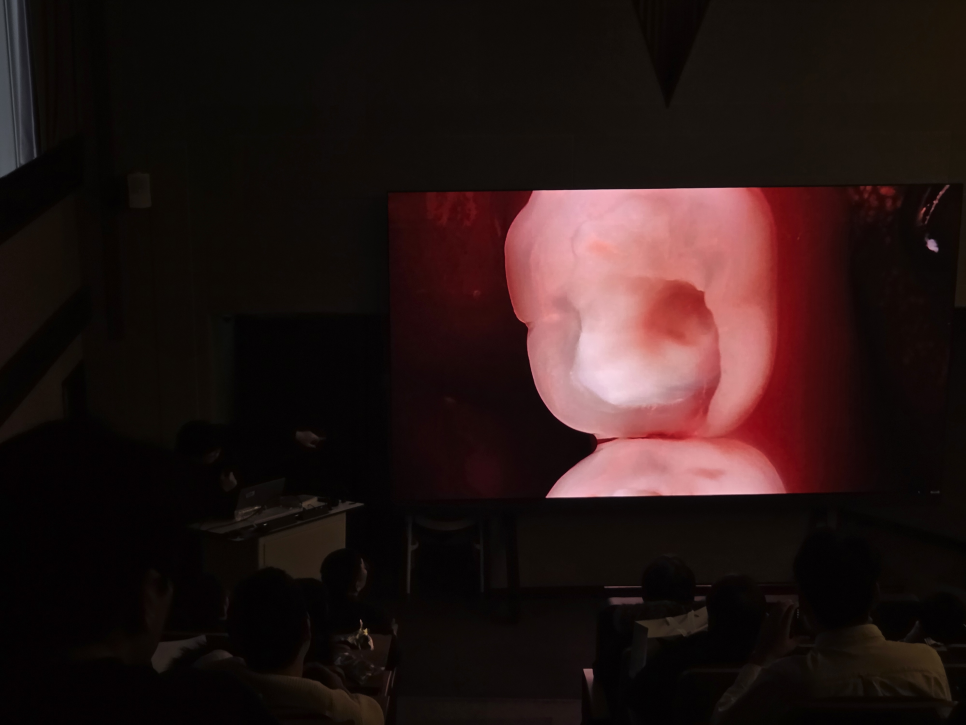
It is equipment that helps leave healthy tooth structure in place
and remove only the cavity accurately.
If you treat using only the naked eye,
it can be difficult to accurately distinguish the boundary between decay and healthy tooth structure,
which can lead to unnecessary removal.
But when you use Qray,
that boundary becomes clearly visible.

As this kind of experience accumulates,
you can reduce unnecessary removal,
and as a result, there are clearly cases where root canal treatment does not need to be performed.
In fact, there have been quite a few cases where patients came in after being diagnosed at another clinic with a need for root canal treatment,
but the case was completed with minimally invasive resin treatment using Qray^^
The meaning of avoiding root canal treatment
During the lecture, I also said that "root canal treatment is a blind treatment."
The expression may sound a bit blunt,
but the meaning is clear.
No matter how well it is done,
root canal treatment is a procedure where it is difficult to immediately confirm whether it has succeeded.

So if possible,
I believe finishing treatment at the crown portion is better care for patients.
That is why I use Qray to reduce unnecessary removal,
and focus on adhesion and sealing while preserving as much remaining tooth structure as possible.
This does not mean that root canal treatment should never be done,
but rather that if there is a way to avoid it,
I want to think about that path first.
Anterior resin is not about color,
but about structure
What I emphasized most while talking about anterior resin in this lecture
was that "resin is not a treatment done with color."
The incisal edge halo, dentin mamelons, translucent layer, and curvature...
all of these elements are not problems solved by changing the resin color;
they are questions of how to understand and reproduce tooth structure.
That is why, before talking about materials,
I always first talk about "what structure in this tooth should be preserved."

This is the biomimetic approach that I pursue,
and it is the core principle I value in anterior treatment.
Resin is not an easy treatment,
but a treatment that requires choices
As I honestly said during the lecture,
resin treatment is by no means easy.
Because you have to restore the texture of the tooth one layer at a time,
it takes a long time,
and depending on the clinician's concentration and experience,
even the smallest difference in outcome becomes very clear.
To be honest,
for the doctor, it is a very labor-intensive treatment.
The more time and care the doctor invests,
the more safely the patient's tooth can be preserved.
What I consider good treatment is
explaining transparently the amount of tooth removal, the aesthetic result, and the pros and cons of each treatment,
and helping the patient make the choice they will regret the least on their own.
That is why, even while taking the difficult path of "minimally invasive" care, I try to communicate with patients at every moment.
(That is why my consultation times are very long^^;)

Once again, thank you to everyone who attended the lecture.
After a lecture ends, I always have the same thought.
"In the end, the destination of all this learning
must be back in the treatment room" haha
A lecture is a place to share well-organized results,
but actual treatment is the fierce process of facing patients with different teeth and different concerns each time,
and finding the answer.

With Dr. Kim Jun-yeob, a master of anterior prosthetics,
and Dr. Jeong Seok-hwan, the lecturer😊
Going forward, I will not focus only on the technique of "resin build-up."
I will continue providing care that fully communicates why this treatment is the best option for the patient,
and care that precisely diagnoses with Qray and preserves natural teeth through minimally invasive treatment.
I hope my sincerity came across well.🙏🏻
Thank you.
👇🏻 Quick Reservation 👇🏻
👇Good posts to read together! 👇