Reference
The Triple Plane, the Bra-Flap, and the Inverted Bra-Flap Modified Dual Plane
Techniques for Breast Augmentation
Roberto Bracaglia, MD; Maria Servillo, MD; Regina Fortunato, MD; and Stefano Gentileschi, MD, PhD
Aesthetic Surgery Journal 2020, Vol 40(4) NP141–NP151
Animation deformity that may appear after breast surgery is more accurately understood not simply as a side effect that occurs only when the surgery was performed incorrectly, but as a structural phenomenon that appears depending on how the implant and the pectoralis major muscle are positioned in relation to each other.
Recently, as procedures such as the triple plane method have introduced different ways of designing muscle separation and implant support structures, I believe interpretations of animation deformity also need to be discussed in a more detailed, evidence-based way.
This article summarizes, based on a paper that includes 20-year long-term follow-up clinical data, what kind of problem the triple plane method was developed to address and by what standards animation deformity should be judged.
Animation deformity is not an “abnormality,” but a structural issue.
Animation deformity refers to the phenomenon in which, after breast surgery, the implant or the breast shape appears to move together when the arms or shoulders are moved due to contraction of the pectoralis major muscle.
If the implant is placed in a position adjacent to the pectoralis major muscle, some degree of movement can occur with any technique. This is closer to a phenomenon arising from anatomical structure than to an abnormal complication.
Clinically, what matters is not simply whether animation deformity is present or absent, but also how severe it is, whether it affects daily life or satisfaction, and whether it is likely to worsen over time.
Animation deformity cannot be explained by a single procedure.
When studies and clinical data are combined, animation deformity is difficult to explain by one specific technique alone.
The degree of development of the pectoralis major muscle, exercise habits, the thickness of the skin and soft tissues, the size and weight of the implant, the area and direction of contact between the implant and the muscle, and even the extent of muscle dissection and the incision method all interact in a complex way.
This is why results can differ depending on who undergoes the same procedure and under what conditions.
The triple plane method is not a procedure that simply “works the muscle more.”
The triple plane method was proposed to structurally improve implant palpability and animation deformity, both of which had been pointed out in the conventional dual-plane technique.
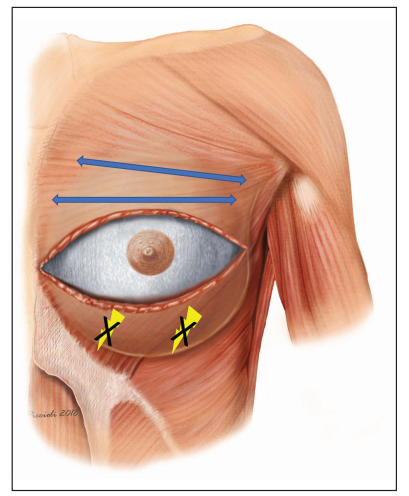
The key to this technique is horizontally separating the pectoralis major at the nipple level and rearranging the muscle contraction direction and the implant support structure.
The triple plane structure is composed as follows.
-
The upper portion covers the implant beneath the pectoralis major to soften the contour
-
The middle portion opens the muscle to secure projection below the glandular tissue
-
The lower portion supports the implant beneath the Bra-flap formed by the lower pectoralis major, serratus anterior, external oblique, and rectus sheath
In other words, it is a method designed by dividing the purpose by layer: coverage in the upper portion, shape in the middle, and support in the lower portion.
The bra-flap modified dual plane and the inverted bra-flap modified dual plane derived from this concept are also selectively applied depending on soft tissue thickness and the degree of ptosis.
At our hospital, we explain this multi-plane concept to patients in an easy-to-understand way using the term triple plane method.
Results shown by 20-year long-term follow-up data
The referenced paper contains results from long-term follow-up of a total of 605 patients over more than 20 years.
As a result of applying the triple plane and bra-flap techniques,
no structural complications such as bottoming-out or double bubble were reported.
In addition, by horizontally incising the pectoralis major and changing the direction of muscle contraction to a horizontal one,
severe animation deformity in which the breast lifts upward or becomes distorted during muscle contraction was reported at 0%.
The BREAST-Q questionnaire also showed significant improvements in appearance satisfaction and psychosocial and sexual well-being compared with before surgery.
Concerns about bottoming-out and extensive tissue damage
Concerns raised by some about the triple plane method show conclusions that differ from the empirical data in this paper.
The bra-flap, which is the core of the triple plane method, is a muscle-fascia composite support structure that includes not only the lower pectoralis major but also the serratus anterior, external oblique, and rectus sheath.
It functions like a hammock supporting the implant from below and structurally blocks the vertical muscle contraction direction known to be a major cause of bottoming-out.
In addition, the triple plane method is designed to minimize unnecessary dissection of glandular tissue and reduce situations in which the muscle rolls upward and compresses the implant.
It is closer to an anatomical design for securing long-term stability than an approach intended to increase tissue damage.
The paper clearly states in conclusion that the triple plane method is not a universal technique that should be applied to every patient.
However, it emphasizes that it can be a very effective option in cases requiring lower support, such as patients with thin skin, constricted breasts, or complex revision surgeries.
The key point is that long-term clinical results of more than 20 years demonstrated that, depending on how the pectoralis major is divided and repositioned, implant visibility can be reduced while support can be maximized.
At Eua Plastic Surgery, we study and apply the triple plane method in ways that minimize tissue damage in order to achieve more natural and stable results, and many patients are satisfied with the outcomes.
Rather than presenting a specific procedure as the correct answer, I believe the most important thing in breast surgery is to choose the most appropriate pocket by considering the patient’s anatomical structure, lifestyle pattern, and the changes that occur over time.
What I would like to say
I organized this article while observing up close the efforts of the medical team at Eua Plastic Surgery, who have continuously studied and refined their techniques to provide patients with the most natural and safe results.
I also understand that recent concerns about certain techniques arise from a desire to care for patients.
However, it is regrettable when sufficient research and long-term clinical outcomes are not conveyed together.
Techniques such as the triple plane method are not merely methods that work the muscle more, but the result of considering how to anatomically overcome the existing limitations of bottoming-out and animation deformity based on more than 20 years of follow-up data.
I believe this is not an approach that increases tissue damage, but a design intended to reduce unnecessary deformity and secure long-term stability.
I believe medicine advances when it is discussed calmly based on evidence and clinical experience, rather than judged from brief information.
Rather than judging one another based on short snippets of information, I hope we can work together toward the essential values of natural beauty and patient safety.
I would like to express my sincere respect and support for all medical professionals who are working behind the scenes to change patients’ lives.