On August 28, 2025, I attended Professor Park Eun-cheol’s lecture on “medical fees” in the Korean Medical Association’s Medical Policy Advanced Course. The conclusion was simple.
If the calculation method changes, the field changes.
A fee schedule is ultimately a signal system that determines “what direction healthcare should move in.” The fairer and smarter that signal is, the less patients, medical staff, and finances all suffer.
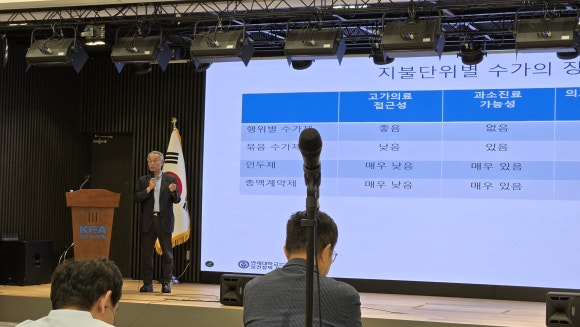
The way medical costs are calculated can be summarized into three types:
-
Item-by-item calculation, adding each item in the basket one by one (fee-for-service)
-
Set calculation, bundling everything together like a course meal (bundled payment)
-
Registration/monthly payment for managing local residents for a certain period (capitation/global budget)
As the unit becomes larger, the insurer’s uncertainty decreases and the provider’s risk increases. That is why, when the unit gets larger, safety mechanisms such as severity adjustment, risk-sharing and reinsurance functions, night-time and emergency add-ons, and performance incentives must be attached.
The components that make up the fee schedule were also explained in an easy-to-understand way.
-
Classification: the standard for deciding what to group and separate by
-
Relative value points: fairness in difficulty, time, and resource use
-
Conversion factor: the exchange rate applied to the points
-
Adjustment factors: compensation for difficult situations such as night shifts, holidays, emergencies, and essential care
When these four parts work together, distortion decreases. If even one is off, behavior tends to tilt in one direction or necessary care gets pushed aside.
The professor explained that in the United States, hospital costs are paid as an “inpatient episode package,” while physician compensation is calculated separately according to the “difficulty and time of the procedure,” and that this separation balances each side by checking excesses and shortfalls. He also said that in our reality, the new bundled payment system, which is a practical compromise between the two (a hybrid model in which inpatient and basic care costs are settled as one bundle, while physicians’ specialized services such as surgery and procedures are reimbursed separately according to difficulty and time), is more realistic.
However, he emphasized that the current new bundled payment system has low participation because its billing rules are excessively complicated and profitability is unclear. Unnecessary complexity should be sorted out, and night-time, emergency, severe, and essential-care services should reflect sufficiently meaningful add-ons that are actually felt in practice. The key is not to rely on goodwill, but to change behavior through numbers and compensation.
I completely agree. Hospitals are always more tiring and dangerous at night and on holidays. If we still have to save patients during those hours, then we need to create a numerical reason to choose that time. Compensation should not be for show; it should be enough that a doctor would voluntarily take on the duty shift. To get people moving, the system must be designed so that both individuals and hospitals clearly feel the benefit when they participate in night, emergency, and severe-care treatment. Also, regulations that limit certain procedures to only a small number of people should be eased so more personnel can share the work, and staffing, facility standards, and compensation should be revised accordingly to reduce gaps. In the end, the force that moves essential healthcare is not goodwill but institutional incentives..
The key is to distinguish between “equity” and “level.”
“Equity” means giving similar compensation for the same effort and difficulty, while “level” means adjusting the overall height of compensation (the unit price per point) so that it is neither too low nor too high. For example, if an ultrasound of the same difficulty is performed, it should receive a similar price wherever it is done (equity), and the overall average should be adjusted so that the price itself is not excessively low or high (level).
As things stand, when the unit price per point differs by field, the gaps are likely to become fixed. The solution is to gradually converge toward one standard, and to reduce the shock of change, the relative value points can be adjusted during the transition period so the shift is smoother.
Finally, to avoid having to pull back and forth every time, if the system includes a rule for automatic readjustment every two to three years based on data, then numbers rather than words will keep the balance.
The move from procedure-centered care to “person- and outcome-centered care” was also compelling. In areas where repeated and continuous management is key, such as chronic disease, patient-registration-based primary care and capitation fit well. In areas where the quality of precise diagnosis and treatment is what determines success, outcome-based compensation is appropriate. The field becomes rigid when it is forced to accept only one answer. A “mixed operating model” that embraces the principle of continuous care = patient-based, precision care = outcome-based, and fast/simple care = procedure-based is what fits Korea’s healthcare structure. That is why we need the basic policy routine of continuously testing a “primary physician registration system,” a “responsible medical alliance” in which local medical institutions are grouped into teams that share responsibility for both cost and outcomes, and “performance-based compensation” that pays more when outcomes are achieved and less when they are not, and then quickly expanding designs whose effectiveness has been verified. A system stays alive only when it is continually adjusted, and to stay alive it must never stop being tested.

Personally, the simplification of the new bundled payment system seemed necessary. The idea is to rewrite the rules more simply and leave only the minimum necessary billing codes and indicators so that everything aligns to one standard. If things are complicated, even those who work sincerely make mistakes, and the system’s purpose becomes blurred. Next, a new “add-on schedule that is actually felt” needs to be created. Night, emergency, severe, and essential-care services should be compensated enough to actually change the duty roster, while severity adjustment and risk-sharing should be designed together so that the system does not become one that benefits those who do less. Lastly, an environment that reduces the criminal burden in medical malpractice is needed. Civil compensation should be made more sophisticated, but criminal liability should be limited to exceptional situations so that necessary treatment is not hesitated over; only then will the effects of fee reform fully take hold.
The purpose of fee reform can ultimately be summed up in one sentence.
To use a fair calculation method to encourage good choices in the field and return better outcomes to patients
What is needed now is the determination to remove complexity and the courage to compensate boldly where it is needed. When the calculation method changes, our daily life changes. And that change will in turn lead to patient well-being.
Written by: Kim Jin-o, New Hair Plastic Surgery (Director of Public Relations, Korean Society of Plastic and Reconstructive Surgeons / Academic Director, Korean Laser, Dermatology and Hair Society)
 Central University Family Medicine Professor Kim Jeong-ha and Coolman Urology Clinic Director Lee Geun-wook
Central University Family Medicine Professor Kim Jeong-ha and Coolman Urology Clinic Director Lee Geun-wook
| Item | Key points | One-line note |
|---|
| Broad framework of payment methods | Itemized (fee-for-service), bundled (DRG), registration/monthly payment (capitation) | As the unit gets larger, provider risk rises, so safeguards are essential |
| Essential safeguards | Severity adjustment, risk-sharing/reinsurance, night-time and emergency add-ons, performance incentives | Change behavior through numbers |
| Four components of the fee schedule | Classification, relative value, conversion factor, adjustment factors | Manage equity (value) and level (unit price) at the same time |
| U.S. vs. Korea | U.S.: hospital DRG + physician procedures, Korea: new bundled payment (bundle + add-on orders) | Balance comes from separation and compromise |
| Challenges of the new bundled payment system | Complicated billing and uncertain profitability reduce participation | Restore incentives by simplifying rules and adding add-ons people can feel |
| Conversion factor | Field gaps become fixed | Gradual convergence, and adjust RVUs during the transition |
| Essential healthcare | Real compensation for nights, holidays, and severe cases | Enough to change the duty roster |
| Next step | Mixed model centered on people and outcomes (primary physician, ACO, P4P) | Ongoing pilot programs, rapid expansion of effective designs |
| | | |