
Female pattern hair loss (FPHL, Female Pattern Hair Loss) is more than just a cosmetic issue of reduced hair volume; it directly affects quality of life.
However, treatment options are still limited, so one of the questions patients ask most often is:
Can women also take male pattern hair loss medications (finasteride, dutasteride)?
A recent analysis using large-scale data has provided a meaningful answer to this question.
Female hair loss, male hair loss medications (finasteride·dutasteride)
Is it safe to use? Summary of the conclusion

Source - Health JoongAng
Finasteride

Source - Pharm News
Dutasteride
The use of male pattern hair loss medications in female pattern hair loss is not yet an officially approved treatment, but large-scale data analysis is reducing major concerns about safety.
In particular, it may open up a new possibility for patients who have not achieved satisfactory results with minoxidil alone.
That said, a thoroughly individualized approach is needed based on the patient’s age, reproductive plans, and personal risk factors.
Q1. Can androgen inhibitors also work for female hair loss?
Women are also affected by male hormones (androgens).
In particular, DHT (dihydrotestosterone) acts on hair follicles and gradually makes hair thinner and weaker, and this mechanism is observed not only in men but also in women with hair loss¹².
Therefore, 5-alpha reductase inhibitors such as finasteride and dutasteride have theoretical value for female hair loss as well.
In fact, some clinical reports have shown cases in which hair thickness and density improved when these two drugs were used.
Q2. Then why are they not officially approved for women yet?
At present, the only drug officially approved worldwide for the treatment of female pattern hair loss is minoxidil.
The reason finasteride and dutasteride have not been approved is the lack of safety data, especially concerning the potential risk to a fetus in women who could become pregnant.
Therefore, their use in women has always been off-label.
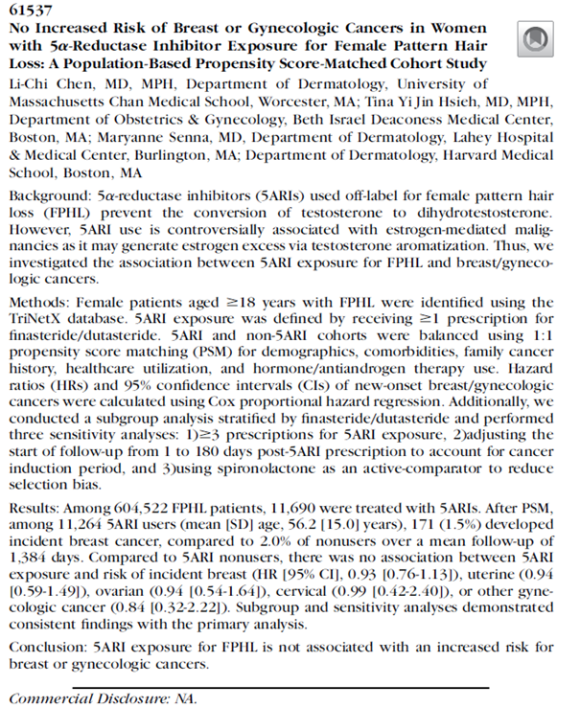
Q3. What were the results of the recent large-scale data study?
There was a study analyzing TriNetX network data from the United States, based on electronic medical records from millions of people³.
-
Study population: about 600,000 female patients with female pattern hair loss
-
Among them, 11,690 took 5-alpha reductase inhibitors
-
Average follow-up period: 3.8 years
The analysis found no difference in breast cancer risk between the two groups (HR 0.93, 95% CI 0.76–1.13), and no increased risk was observed for other gynecologic cancers such as uterine, ovarian, or cervical cancer.
In other words, in large-scale real-world clinical data, there was no evidence that taking these drugs increased the risk of cancer in women with hair loss.
Q4. Then can all female patients take them without concern?
Not quite. There are important limitations.
Women of childbearing potential: because these drugs may affect the sexual development of a male fetus,
use in women who could become pregnant should be approached with extreme caution, and reliable contraception is essential.
Long-term safety: because the average follow-up period was only about 3 to 4 years,
safety with long-term use beyond 10 years still requires further study.
Therefore, in clinical practice, they may be considered in a limited way for postmenopausal women or women for whom adequate contraception is assured.
Q5. How can this be applied in actual clinical practice?
I explain it to patients like this:
If minoxidil alone has limitations, recent research suggests that medications such as finasteride or dutasteride may be cautiously considered.
However, it is important to provide individualized treatment after fully evaluating each patient’s hormonal status, pregnancy plans, family history, and other factors.
Female hair loss, male hair loss medications (finasteride·dutasteride) Is it safe to use? Summary table
| Category | Content |
|---|
| Study population | About 600,000 female patients with FPHL (11,690 5ARI users) |
| Follow-up period | Average 3.8 years |
| Main result | No increased risk of breast, uterine, ovarian, or cervical cancer |
| Breast cancer HR | 0.93 (95% CI 0.76–1.13) |
| Clinical significance | A possible option to supplement the limitations of minoxidil |
| Caution | Women of childbearing potential: fetal risk → contraception is mandatory |
Now it’s time to grow hairhair, this is Kim Jin-o.
Becoming new hair (必生新毛).

Written by: Kim Jin-o of New Hair Plastic Surgery (Public Relations Director, Korean Society of Plastic and Reconstructive Surgeons / Academic Director, Korean Society for Laser, Dermatology and Hair)
References
-
Ho CY, et al. (2023). Female Pattern Hair Loss: An Overview with Focus on the Role of Dihydrotestosterone and Androgen Receptors. PMC. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC10379895/
-
Carmina E, et al. (2019). Female Pattern Hair Loss and Androgen Excess: A Report from the Journal of Clinical Endocrinology & Metabolism. J Clin Endocrinol Metab, 104(7):2875–2883.
-
J Am Acad Dermatol. (2025). No Increased Risk of Breast or Gynecologic Cancers in Women with 5α-Reductase Inhibitor Exposure for Female Pattern Hair Loss: A Population-Based Propensity Score-Matched Cohort Study. DOI: 10.1016/j.jaad.2025.05.267.
[In accordance with Article 56, Paragraph 1 of the Medical Services Act, this post is written directly by a board-certified plastic surgeon for informational purposes. Hair transplant surgery and treatment may have side effects, and decisions should be made carefully through consultation with a specialist.]