Hello.
Today, I’m sharing the story of a patient who came to the clinic for correction of a protruding mouth in their 30s.
Many people worry, “If teeth are extracted, won’t the mouth go in too much?”
However, depending on how the extraction spaces are finished, the attending doctor can control how much the front teeth are moved back.
This is a reminder not to wait until extraction orthodontic treatment is all over, only to feel upset that the mouth has become too sunken or too retrusive and then go around consulting about retreatment. It is important to keep discussing the progress with the attending doctor along the way.

22.09~25.04
Today, I’ll show you how the amount of retraction of the front teeth is controlled during extraction orthodontic treatment for a protruding mouth with lip incompetence.

22.09
This patient in their 30s came in for orthodontic treatment in September 2022.

22.09
They visited to improve the puffy impression caused by protruding front teeth and to correct the inability to close the lips properly.

22.09
We recommended extraction orthodontic treatment with removal of four premolars, and treatment began with the patient choosing Clippy-C orthodontics.
In September 2023, one year after treatment began, with about half of the extraction space still remaining, it was judged that it would be better not to move the front teeth back any further.
So, after discussing it with the patient using lateral cephalometric X-rays and photographic records, we decided to finish the remaining spaces by pulling the molars forward.

The treatment plan was changed so that the front teeth would no longer be retracted and the extraction spaces would be closed by finishing them with the back teeth.

There are anthropological averages and normal ranges in every field of study, but whether those average values suit my face is something I need to check for myself while also listening to the attending doctor’s opinion and looking carefully.
To bring the molars into the extraction spaces, four orthodontic miniscrews are placed in the front, and elastics are used to pull the molars forward. For the molars to move well to the root level without tipping over, biomechanical considerations such as the point where force is applied are essential.
24.06

24.06
As we kept pulling the molars forward one by one, the treatment went beyond the originally mentioned two-year treatment period.
If we had simply retracted the front teeth and closed the extraction spaces, treatment would have ended in two years, but because we needed to preserve the position of the front teeth and bring the molars forward, it took a long time. In particular, when bite force is strong, molar movement is slower, and this was such a case.
After 2 years and 6 months from the start of treatment, the treatment was finally completed.

25.04
The midline is well aligned.

25.04
The bite is also good after extraction orthodontic treatment for protruding mouth and lip incompetence.
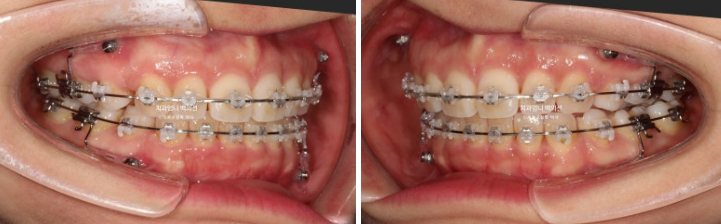
Let’s look at the before-and-after comparison.

22.09~25.04

22.09~25.04

22.09~25.04

22.09~25.04

22.09~25.04
Now let’s look at the facial comparison after treatment for protruding mouth and lip incompetence.

22.09~25.04
The neat smile line and buccal corridor are appealing.

22.09~25.04
Thanks to the changed treatment plan, after the mid-treatment evaluation, the lips were not retracted too much and the treatment was finished well at an appropriate level.

25.04
There is no root resorption, and root parallelism is good.
As the lip incompetence that made it hard to close the mouth because of protrusion has been resolved, the lips now close comfortably.
I hope this helps those who were worried that their mouth might be pulled in too much before undergoing extraction orthodontic treatment for a protruding mouth.