Hello,
This is Apgujeong Orthodontic Clinic.
Today, I’ll talk about skeletal Class III malocclusion.
In other words, when there is prognathism, the front teeth bite in reverse, and the lower lip protrudes.
Even if the skeleton is prognathic, treatment that creates a normal bite through orthodontics alone without double-jaw surgery is called compromise treatment.

24.01~25.06
Today, I’ll show how prognathism and malocclusion were treated with compromise treatment in a case where one premolar, or small molar, was congenitally missing, without double-jaw surgery or additional premolar extraction.
A patient in their late 30s who came in for treatment of anterior crossbite

24.01
The blue arrows indicate a premolar and molar in crossbite.

An anterior crossbite and edge-to-edge bite are visible, where the upper teeth do not cover the lower teeth.
The molar occlusion is Class III.

The small molar between the white lines is missing, and the surrounding teeth have tipped toward the missing tooth.

The lateral incisor indicated by the blue arrow is smaller than normal.
It is not to the point of being a peg lateral, but it is small.
If the two small lateral incisors are enlarged in size with laminates, etc., it would be possible to create an occlusion in which the upper teeth cover the lower teeth more clearly, but the patient does not want that.

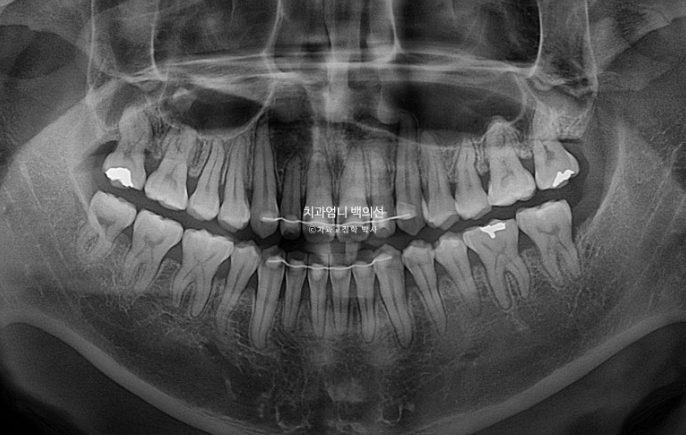
24.01
There is one missing premolar in the blue-arrow area.
Looking at the overall treatment plan, the main goal is to move the lower anterior teeth backward, bring the molar occlusion to Class I, and allow the upper front teeth to cover the lower front teeth.
To do this, the lower left wisdom tooth will be extracted, and the wisdom tooth on the opposite side, where one premolar is missing, will not be extracted.
Although it is somewhat disadvantageous to move the teeth into the wisdom tooth space, this is done to balance the number of teeth on the left and right sides.
The patient chose Clippy-C orthodontics, and treatment began.
In Class III malocclusion, there is a lot to do on the lower dentition and it takes a long time, so we usually start with the lower arch first for at least 6 months, and then begin attaching appliances to the upper dentition, which takes relatively less time. That way, the appliance period is shortened and the patient is more comfortable.
In this case as well, appliances were attached only to the lower teeth for the first 7 months, and then appliances were attached to the upper teeth after 7 months.
This is what it looked like 10 months after treatment began. Mini-screws, which are orthodontic screws, were placed in the lower jaw and the teeth were moved into the wisdom tooth space.

24.11

Treatment was completed 1 year and 5 months after treatment began.

25.06
The midline is well aligned, and the crossbite on one side of the molars has improved without separate arch expansion.

24.01~25.06
The molar that had tipped toward the missing premolar was uprighted well.

The bite is good.

24.01~25.06
The alignment is also good.
The lower wisdom tooth that was left in place is also occluding well.
Now, let’s compare before and after.



24.01~25.06
As the entire lower dentition moved backward, the lower front teeth were brought back, and as a result, the lower lip moved back and lip balance improved.
There is no root resorption, and root parallelism is good.
Good results can be achieved with compromise treatment alone, without additional extraction or double-jaw surgery.
I hope this post is helpful for those who are hesitant about orthodontic treatment because of prognathism.