Hello,
This is Apgujeong Orthodontic Clinic.
Today, I’d like to introduce an underbite, also known as a skeletal Class III malocclusion.
In cases of skeletal Class III malocclusion, depending on the degree, double-jaw surgery may be necessary.
In particular, even among underbites, a divergent facial type with a long lower face vertically often requires double-jaw surgery even more.

24.01~25.07
However, if the patient strongly refuses surgery to the point of saying, “If I have to undergo double-jaw surgery, I’d rather just live without orthodontic treatment,” then treatment may be performed to improve the bite with orthodontics alone.
Today, I’ll show you how non-surgical underbite malocclusion treatment is carried out with Invisalign.

24.01
This is a patient in their 30s who visited for orthodontic treatment 1.5 years ago.
They had received an orthodontic consultation long ago and were advised to undergo double-jaw surgery, so they had given up on orthodontic treatment. Then, when they came in for a family orthodontic consultation, they received a consultation together.
Not only the front teeth but also the molars are in crossbite.
The midline of the front teeth is deviated by about 2 mm.

The molars also show a severe Class III bite relationship. The front teeth are biting in reverse with a crossbite.

24.01
One upper left molar is an implant, and the front teeth are crowded and uneven.
In underbite malocclusion, the alveolar bone supporting the lower front teeth is often thin.
That means the risk of black triangles is also high. Interproximal reduction would be performed to improve this area, but to some extent, black triangles still have to be anticipated.
Although double-jaw surgery was needed, if there is absolutely no intention to undergo surgery, a compromise treatment that at least normalizes the bite can be considered.
Because the underbite is quite severe, there are naturally limitations to normalizing everything with orthodontics alone without double-jaw surgery, but it would still be a much better option than staying as is.
The entire lower arch is planned to be pushed backward using the space from the wisdom teeth, so that the lower front teeth move back and the front tooth bite is normalized.
The patient chose Invisalign, and treatment began.

24.11
The first set of appliances consisted of 45 aligners.
One mini screw, an orthodontic anchorage screw, was placed on each side in the lower jaw, and a prescription for elastics that the patient can remove and put back in on their own was also included.
This is what the patient looked like after wearing all the aligners over 11 months.

24.11
The crossbite of the front teeth has been resolved, and black triangles created as the lower front teeth were aligned are visible.

24.11
The molars are still floating, and the bite is not closing well yet.

Elastic buttons are attached on the inside as well to correct the rotation of the premolar connected to the mini screw.
Additional appliances were remade to improve the remaining issues, and after wearing all 25 additional aligners from December 2024 to June 2025, treatment was completed.

The black triangles are unfortunate, but the midline is almost aligned and the bite has become neat.

24.01~25.07

The crooked front teeth have become aligned.
Now let’s look at the before-and-after comparison. The total treatment period was 1.5 years, and one remake was done.

24.01~25.07
Not only the front teeth but also the molar crossbite improved.
The midline improved.

24.01~25.07

24.01~25.07
Now let’s look at the facial changes.

24.01~25.07
A more organized smile line and an improved smile

24.01~25.07

24.01~25.07
The lower lip moved backward, and compared with the beginning, the lip line looks more harmonious.
24.01~25.07
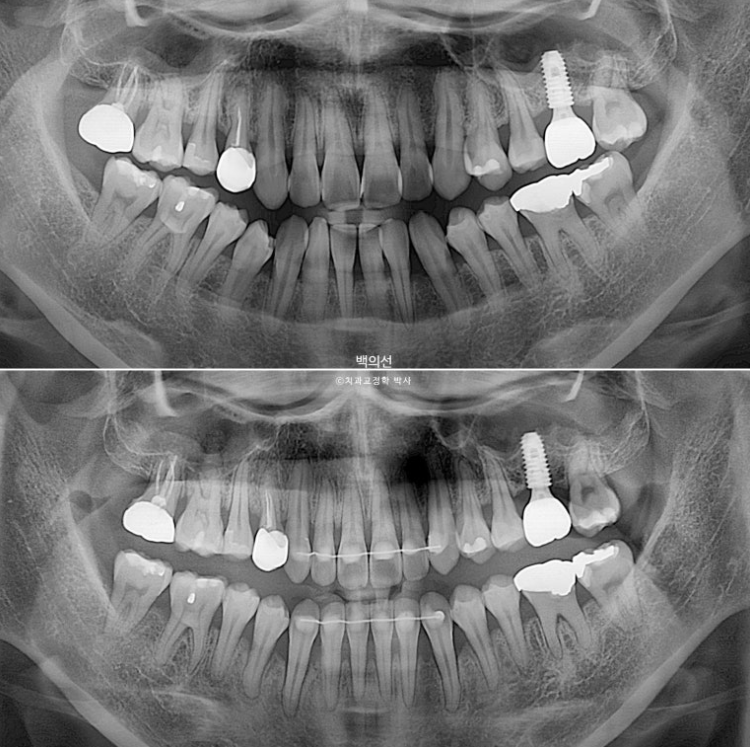
During the 1.5-year treatment period, there was no root resorption, and root parallelism is good.
In particular, as the lower arch moved backward, you can see that the space for the wisdom teeth decreased significantly.
The upper lip showed no change before and after, and as the lower front teeth moved back, the lower lip followed and moved backward as well.
The patient is carefully wearing the Vivera retainers to prevent relapse thoroughly.
If double-jaw surgery had been performed, skeletal measurements, tooth angulations, and everything else could have been finished closer to normal values, but because the patient was highly cooperative, we were able to achieve a fairly good result without double-jaw surgery.
I hope this post is helpful for those who are hesitant to begin orthodontic treatment because they are afraid of double-jaw surgery.