Hello.
This is Apgujeong Children’s Orthodontic Clinic.
Today, I’d like to introduce pediatric orthodontic treatment.
What has traditionally been used for treating asymmetry in children?
The monoblock.

This is what the monoblock appliance looks like.
Because the upper and lower parts are made as one unit, you cannot speak while wearing it, and it has the drawback of being difficult to wear when you need to breathe through your mouth because of nasal congestion.
The Invisalign pediatric orthodontic appliance includes a feature called Mandible Advance (MA).
This function works in the same way as a monoblock, but it has much greater advantages compared with a monoblock.
The MA feature is usually used to guide lower jaw growth when the lower jaw is small and retruded, but it is also useful for improving skeletal asymmetry.
Today, I’ll show you how this MA feature is used to treat skeletal asymmetry in children.

23.12~25.03
In June 2023, a 7-year-old child visited the clinic for orthodontic treatment.
What we wanted to correct was the asymmetry.
The child came in after being told during a school oral exam that the midline was not aligned and treatment was needed.
We decided to improve the asymmetry using the MA feature of Invisalign First.
However, since the lateral incisors had not fully erupted yet, we decided to delay treatment by a few months.
Treatment can begin even when only the central incisors, or upper front teeth, have erupted, but starting when all four front teeth are present makes appliance fit and treatment progress more stable.
So the child returned in November 2023, and after confirming that all four front teeth had erupted, we performed a detailed examination.
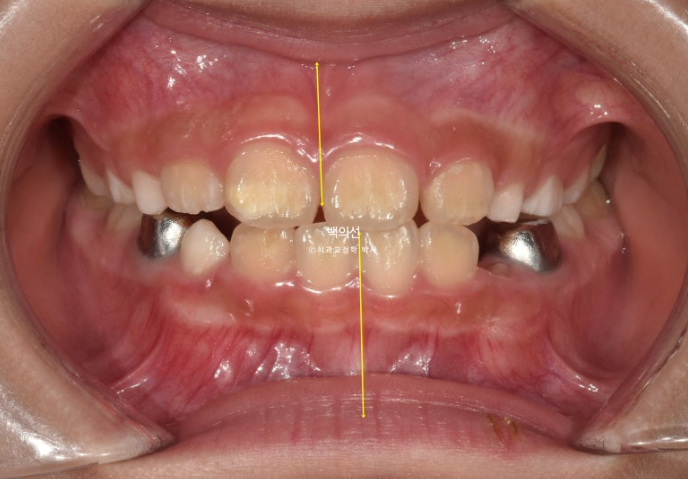
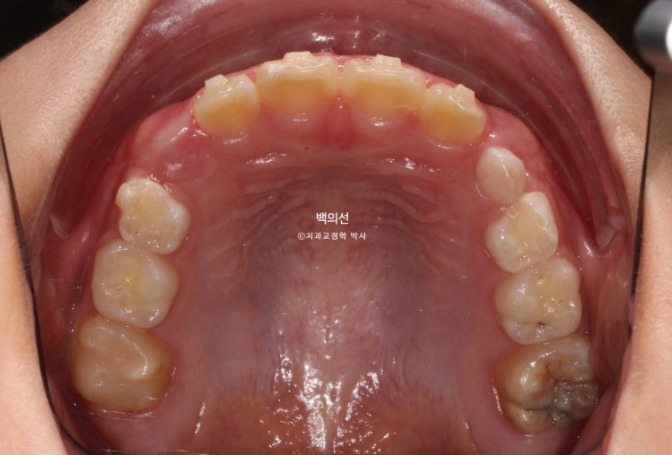
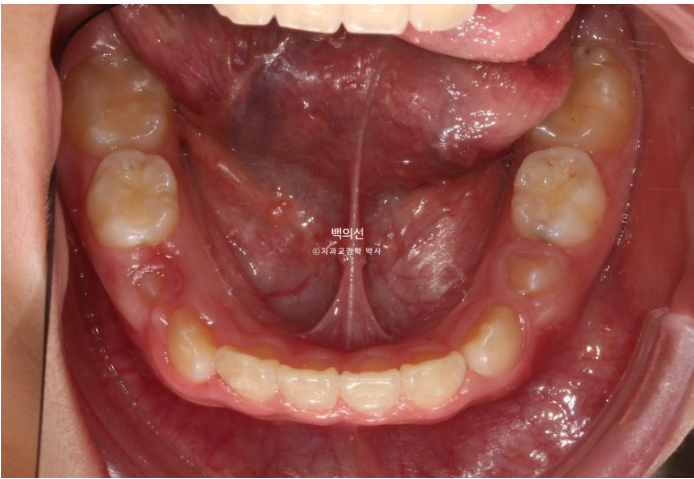
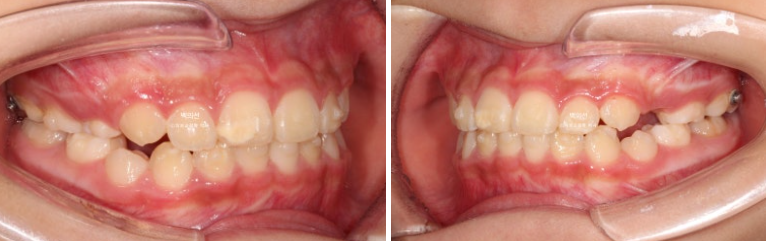
23.12
The front tooth midline was not aligned, and

the X-ray showed skeletal asymmetry of the lower jaw.
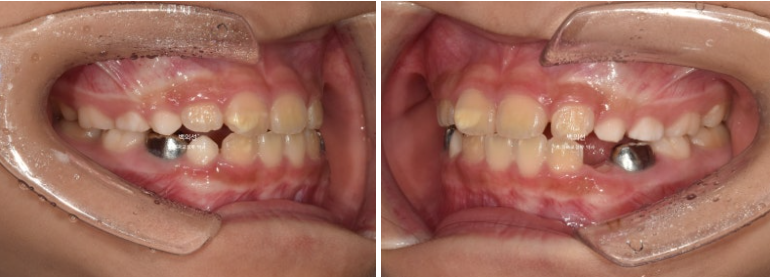


23.12
There was not much space deficiency on this day.
We recommended Invisalign First treatment and made a treatment plan with the goal of improving the asymmetry through the Mandible Advance (MA) feature, which repositions the lower jaw to the center.
Here is this child’s treatment plan.
For the first few months, we first focused on distributing space for the eruption of permanent teeth and improving front tooth alignment, and then from the middle of treatment, the MA feature that guides the lower jaw position was started.
By August 2024, after wearing all 30 appliances in the first set for 9 months, this is the result.

24.08
The midline was well aligned, but the front teeth were in an edge-to-edge bite.
This is because as the twisted jaw position was corrected, the lower jaw rotated to the opposite side and moved slightly forward.
This part needs improvement in the additional appliances.
24.08
24.08
There was adequate space for the permanent teeth to erupt.
We made additional appliances to further align the newly erupted permanent teeth and improve the front bite.
The additional appliances did not include a function to position the lower jaw, and this was a process to check whether the jaw position remained stable after treatment even without MA.
By the time all 16 additional appliances had been worn from October 2024 to March 2025, this was the result.

25.03
The jaw position remained naturally stable for 6 months, and treatment was completed.
The midline is also very well aligned.
25.03
The bite is good, and the first premolar has just started to erupt.

23.12~25.03
Because the treatment result was so good, the retainer was also made like an adult’s, extending from canine to canine.
Although this is pediatric orthodontic treatment, if the result is this good, there is no need for second-stage orthodontic treatment when the child grows up.
Now, shall we look at the facial changes?
The total treatment period was 1 year and 4 months, and one remake was done.

23.12~25.06
The change in the chin tip position is noticeable.

23.12~25.03
The dental midline is well aligned, and

23.12~25.03
The front tooth alignment is also good.

23.12~25.03
The lip line was also well maintained, and

25.03
The root parallelism is good.
At the end of treatment, there are 4 remaining primary teeth, and after they naturally fall out in the future, the permanent teeth will erupt appropriately.
At present, the lower jaw position is stable, so the child is being maintained with only a fixed wire retainer attached, without a removable retainer, and regular checkups at one-year intervals are needed until growth is complete.
If there are signs of asymmetry recurring during growth, a monoblock could be considered as a nighttime-only retainer.
I hope this post is helpful for parents who are considering orthodontic treatment because their child has asymmetry.