Hello.
Today, I’d like to talk about treatment that makes the face appear smaller / intrusion orthodontic treatment.

2209
This patient had orthodontic treatment a long time ago, but came in because of protrusion and difficulty closing the lips, hoping to receive treatment for lip incompetence.
Since the patient had orthodontic treatment in the past, the alignment and bite are good.

2209
When there is lip incompetence, the mouth does not close comfortably, and in order to close it without showing the teeth, the upper and lower lips must remain under tension.
That can be very uncomfortable.
Lip incompetence and a chin dimple are symptoms that occur because the front teeth protrude forward, making it difficult to close the mouth properly.
When the front teeth are moved back through protrusion correction, lip incompetence and the chin dimple naturally improve. But if the degree of protrusion and chin dimple is severe, rather than simply pulling the front teeth back, we treat with intrusion orthodontics that lifts the entire dentition, from the upper front teeth to the molars, so that the lips can close more comfortably.
In orthodontic treatment for people in their 40s and 50s, the main focus is changes in the mouth area, such as nasolabial folds and an elongated philtrum.
Starting around age 35, when soft tissue aging begins, patients over 35 may be at greater risk of having deeper nasolabial folds after extraction orthodontic treatment than younger adult patients.
Many people preparing for orthodontic treatment worry about changes in the mouth area after treatment, such as deeper nasolabial folds and a longer philtrum.
For nasolabial folds to become deeper, the front teeth would need to be moved back a lot, by more than 4–5 mm, as in extraction orthodontic treatment.
In other words, in non-extraction protrusion correction, where the goal is to move the front teeth back only about 2 mm, issues with nasolabial folds are uncommon.

23.07
23.07
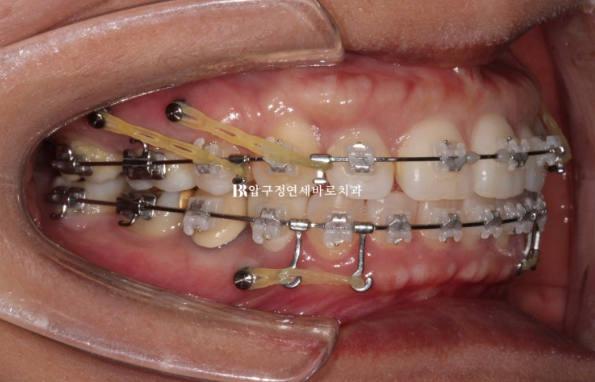
We decided to treat with Clippy-C, placed a total of 6 mini-screws—4 in the upper jaw and 2 in the lower jaw—and proceeded with treatment.
Below, the entire dentition is pushed backward, and in the upper jaw the entire dentition is both pushed back and lifted upward.

22.09~24.04
22.09~24.04
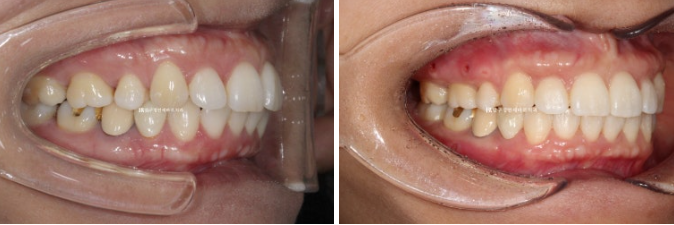
Here is the before-and-after comparison after 1 year and 7 months of treatment.
Since the original alignment and bite were good, there is not much difference in the intraoral photos other than improvement in the angle of the protruding front teeth.
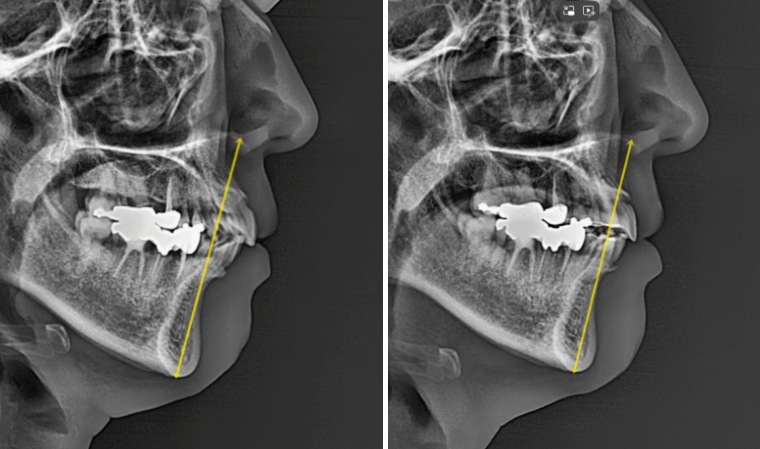
If you look at the superimposed X-rays before and after treatment, the retreatment effect is clearly visible.
With intrusion and posterior movement of the entire dentition, substantial autorevolution of the lower jaw occurred.
In general, treatment aims for about 2 mm, but in this case, about 3 mm occurred.
The area that had looked like a receding chin improved, and the chin dimple relaxed, creating a more natural line from the lower lip to the chin.
When autorevolution occurs, the chin tip moves upward, and from the front the vertical length of the lower face becomes shorter, making the face appear smaller.
Also, due to autorevolution, the chin tip moves slightly forward.
So in cases of a small lower jaw and a receding chin, since the receding-chin appearance also improves, intrusion orthodontics is actively recommended.
However, conversely, if the lower jaw is large and well developed, it is not recommended, because it would be undesirable for the chin tip to move further forward.

22.09~24.04

22.09~24.04
The most noticeable effect is that, by resolving the protrusion, the lips can close comfortably.
The nasolabial folds, which many patients worry about, did not deepen compared with the beginning.
If the front teeth had been moved back more than 2–3 mm, the nasolabial folds might have become deeper than they were initially.