As rhinoplasty using septal cartilage has become more common, there are many cases in which the septal deviation becomes more severe after rhinoplasty.
The human septum may naturally be slightly deviated, but if rhinoplasty is performed without correcting the septal deviation, the nasal deviation often becomes more pronounced.
In the past, the nose was augmented using septal cartilage, but over time the deviation of the nose became more severe.
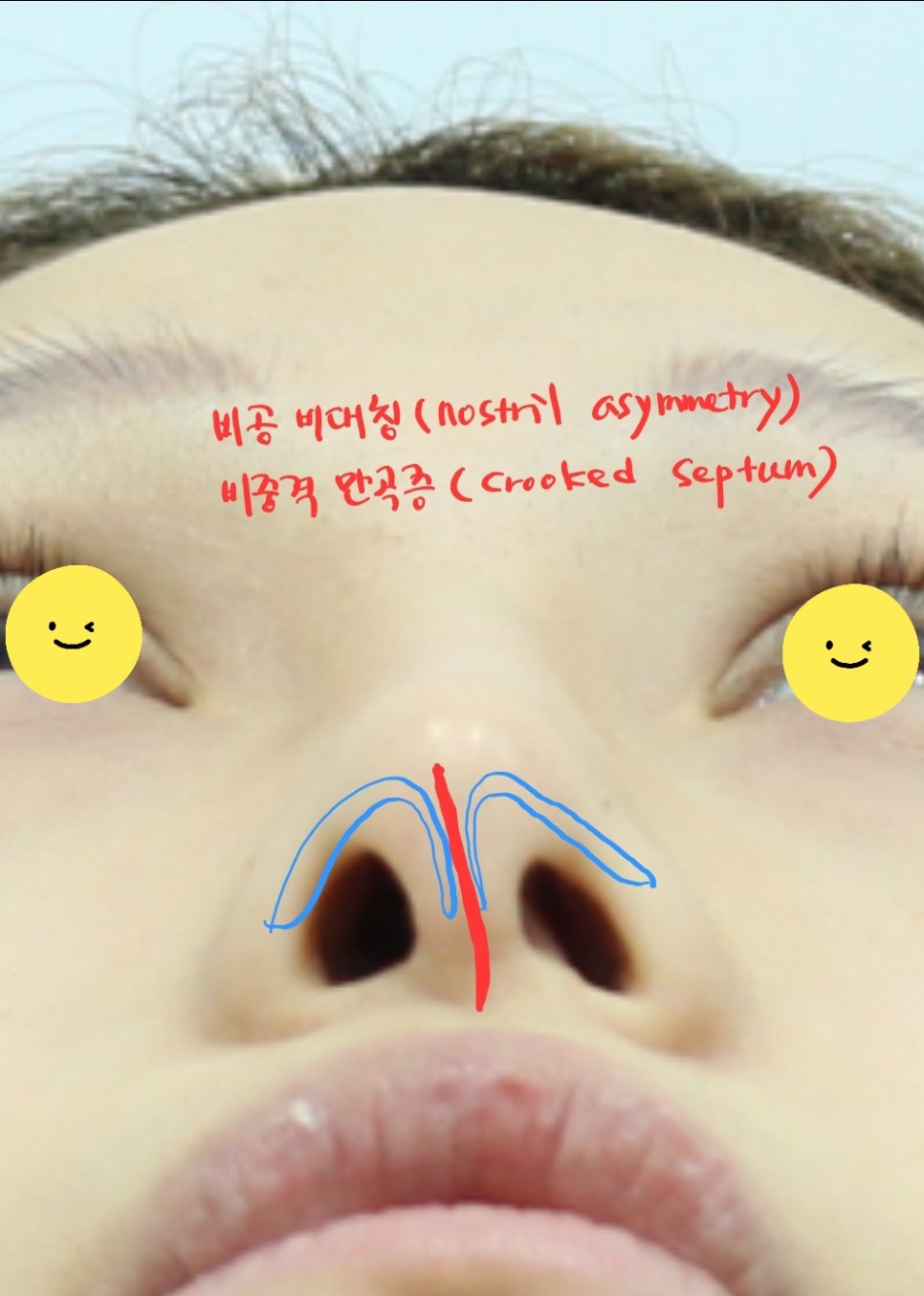
The relationship between nostril asymmetry and septal deviation
When the nose is augmented, the skin of the nasal tip stretches, but if the nasal tip lacks support due to pressure from skin tissue that cannot stretch enough, the tip can droop.
If the septal deviation was not corrected at this time, the nose begins to gradually sink along with the deviation.
From below, the shape of the nostrils changes, and the nasal tip and columella appear to collapse to one side.
In such cases, a CT scan can accurately confirm the internal condition.
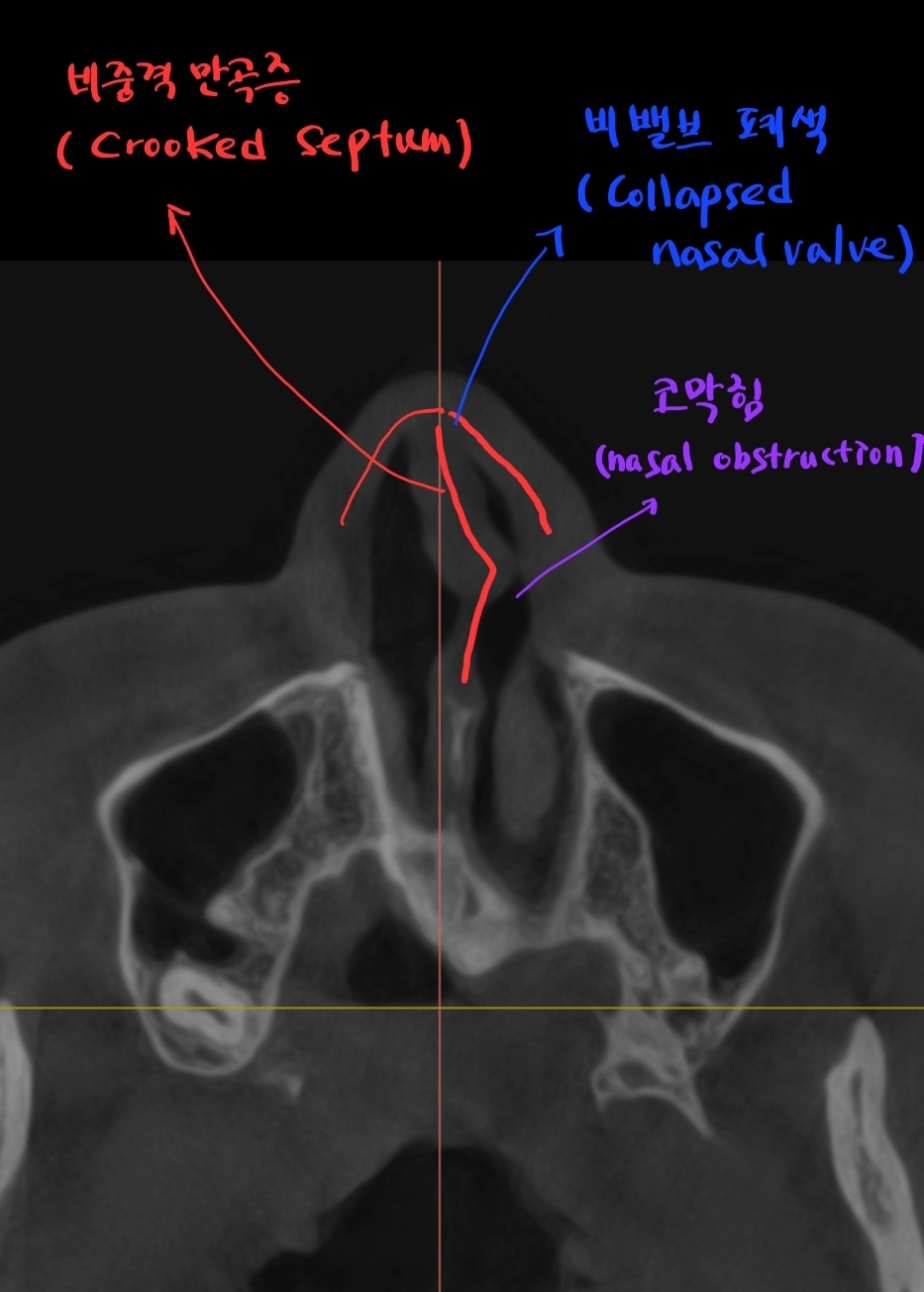
Septal deviation and nasal valve obstruction
The CT results showed that the septum was severely deviated to one side, and one nasal valve had collapsed, causing nasal obstruction.
The patient’s actual symptom was that they could not breathe through one nostril.
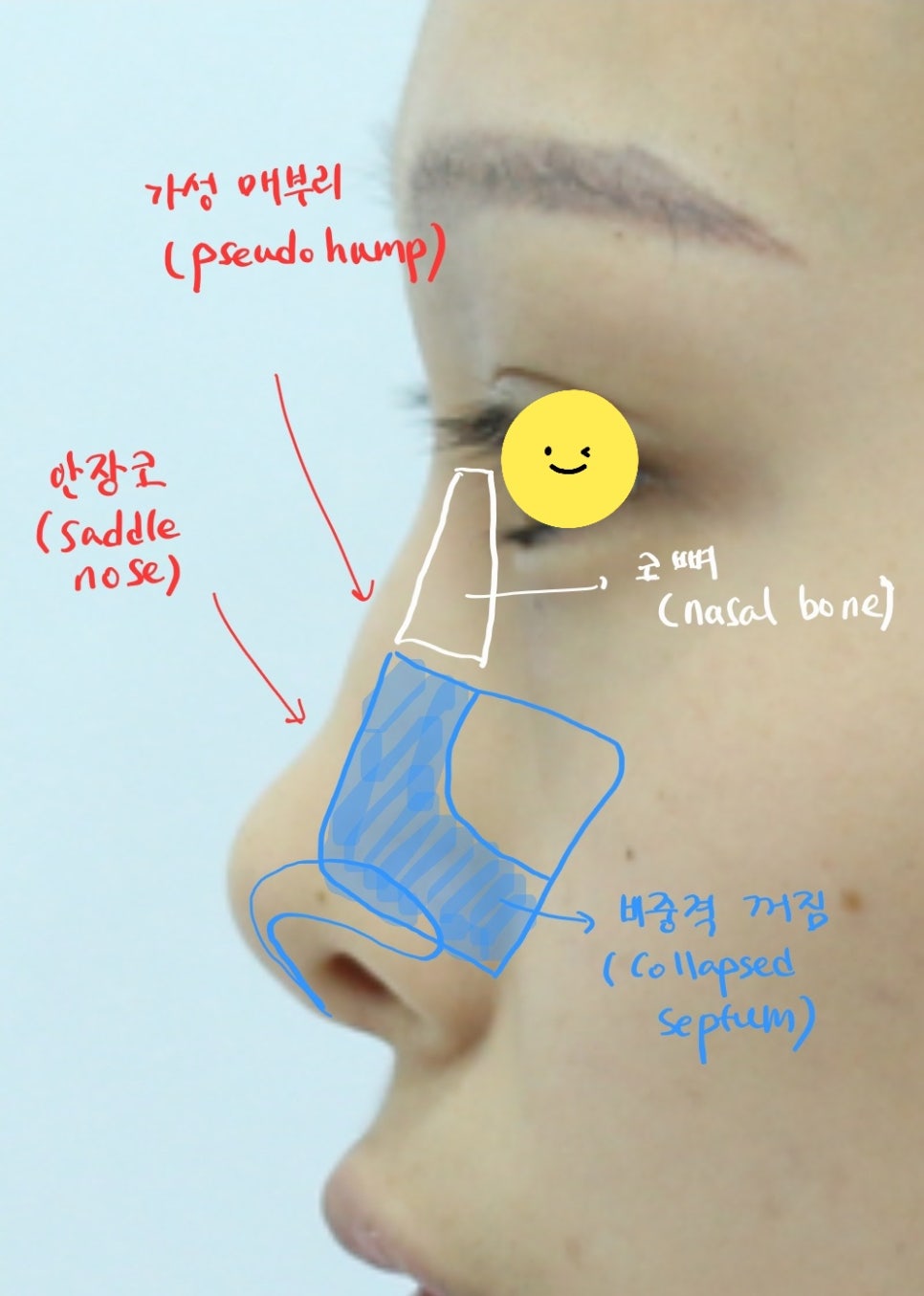
Saddle nose and pseudohump
From the side view, the bridge of the nose appears uneven. A nose like this is called a saddle nose.
Some people mistake this type of nose for a hump nose, but the uneven contour formed by a sunken nasal bridge is correctly called a saddle nose, and the protruding part on top is called a pseudohump.
It refers to a sunken shape, like the saddle needed when riding a horse.

The saddle needed when riding a horse
If the septum has collapsed severely, sufficient cartilage material is needed to raise the nose. The collapsed internal support structure of the nose must be rebuilt and reinforced so that the septal deviation does not recur and the proper nasal height can be maintained.
For this reason, rib cartilage is harvested and used in such cases to obtain enough cartilage material.

Harvested rib cartilage
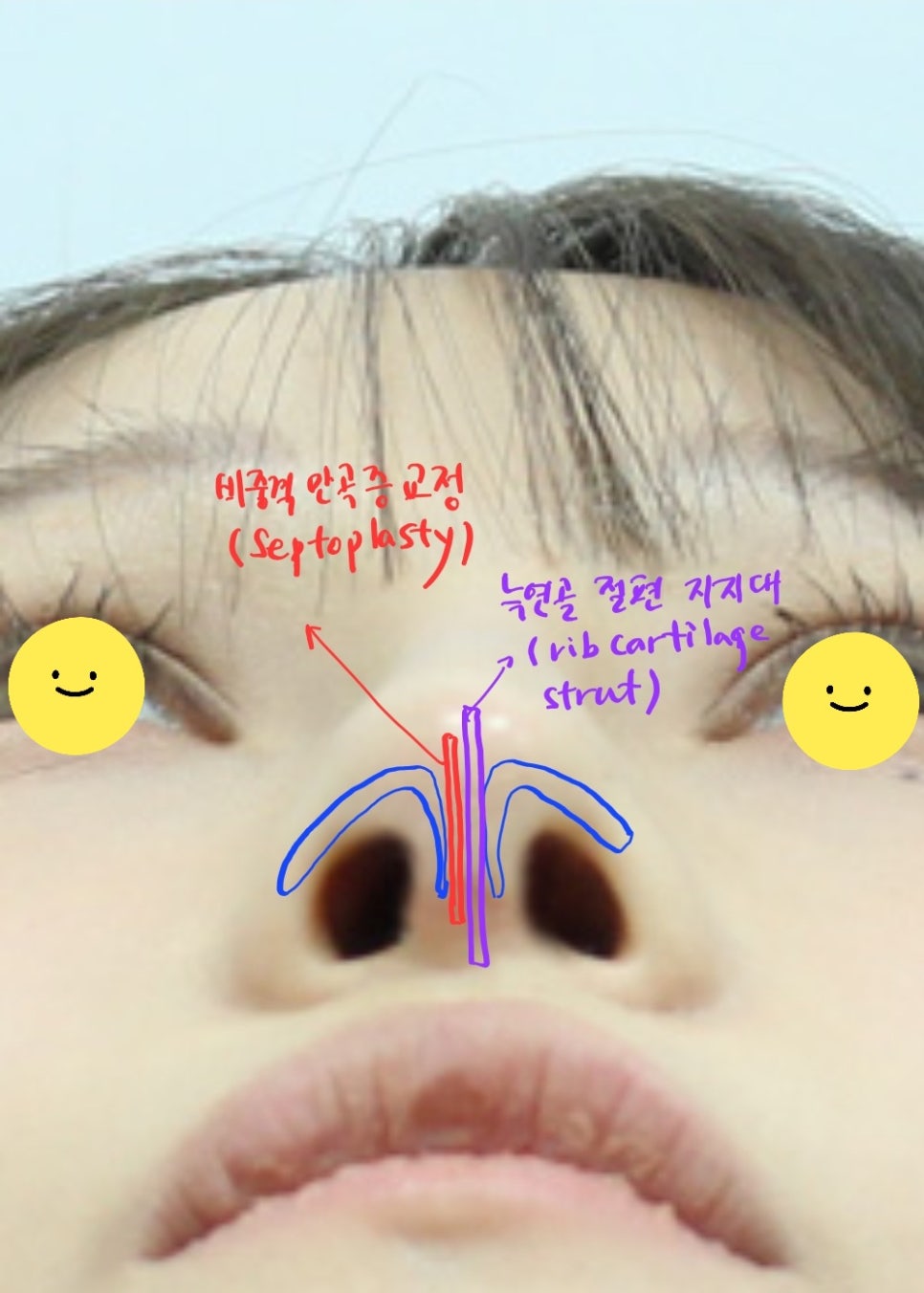
Correction of septal deviation
Using pieces of rib cartilage, the septal deviation is corrected first. Then support cartilage is grafted so that it can firmly support the nasal tip.
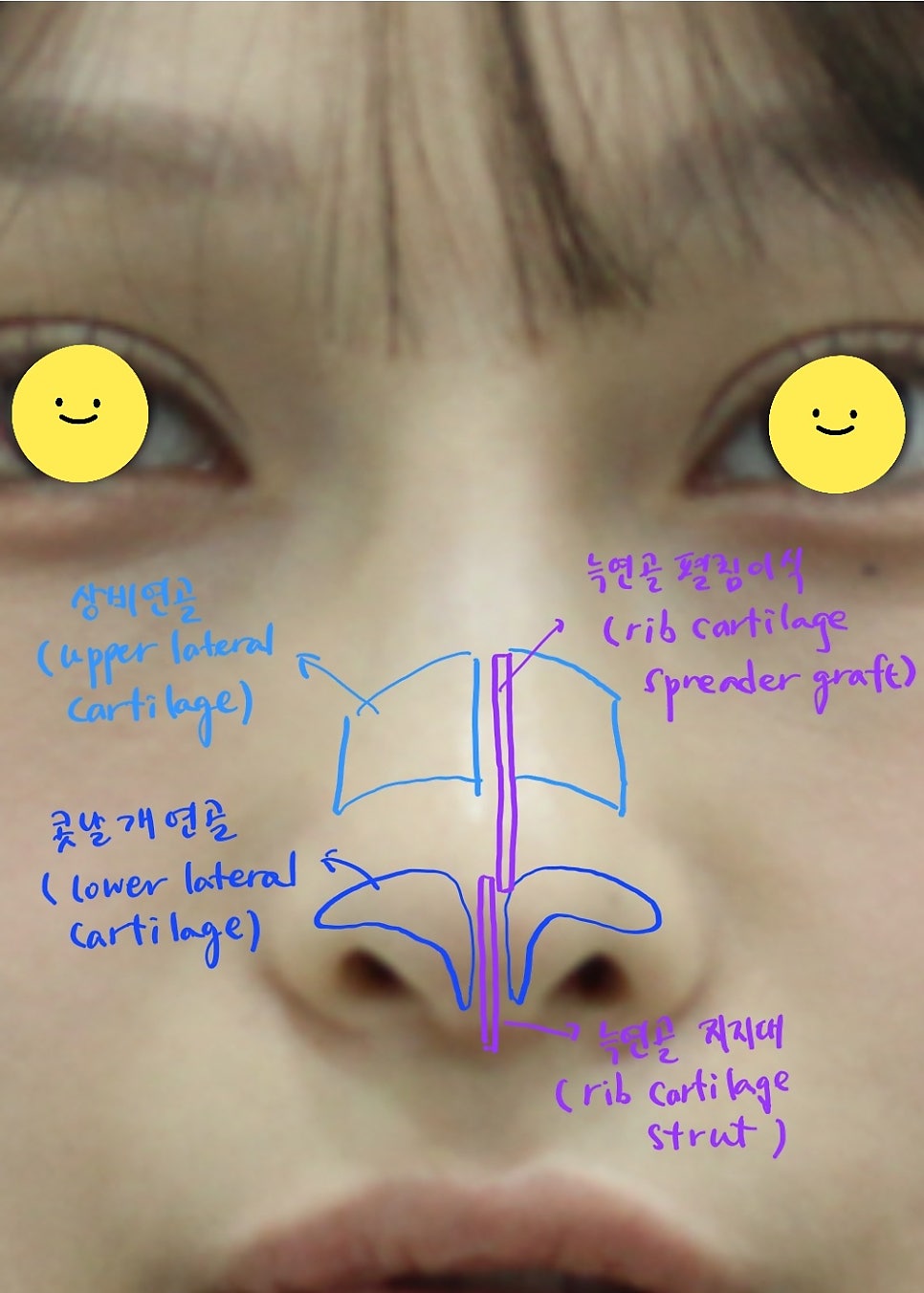
Spread graft using rib cartilage
Then, a spreader graft is performed with rib cartilage pieces on the collapsed nasal valve area. Through this, asymmetry can be corrected and the airway inside the nose can be opened.
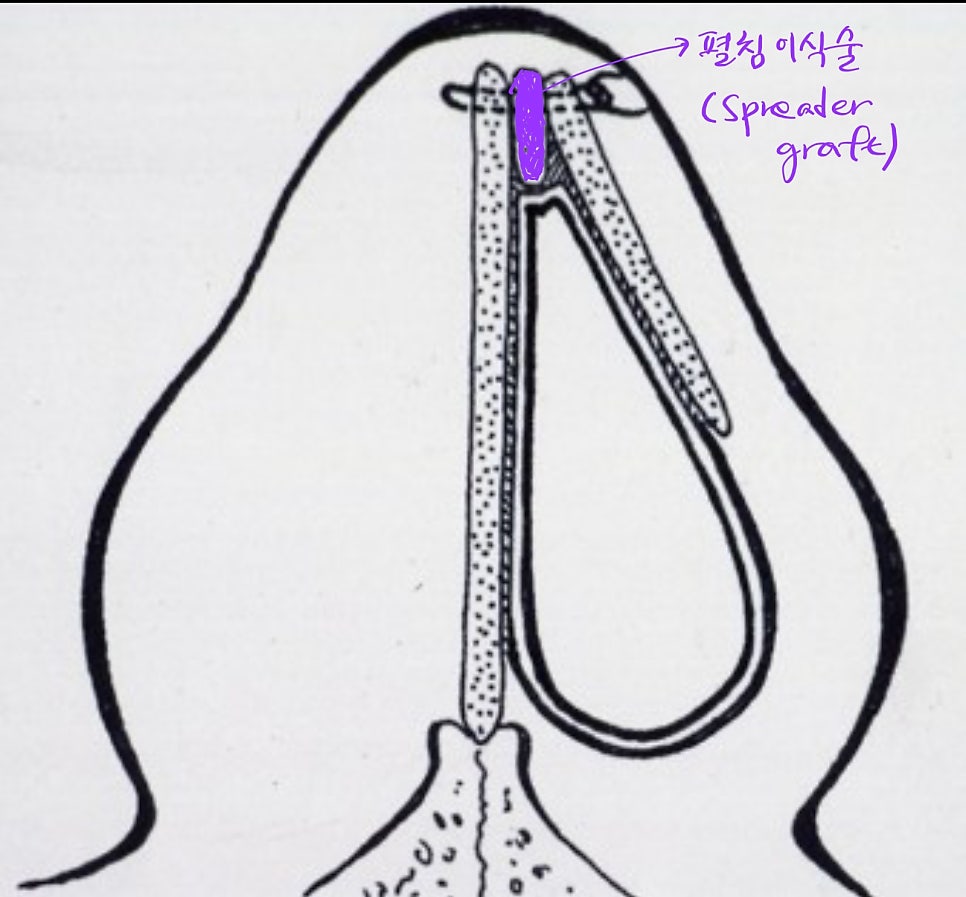
Spreader graft
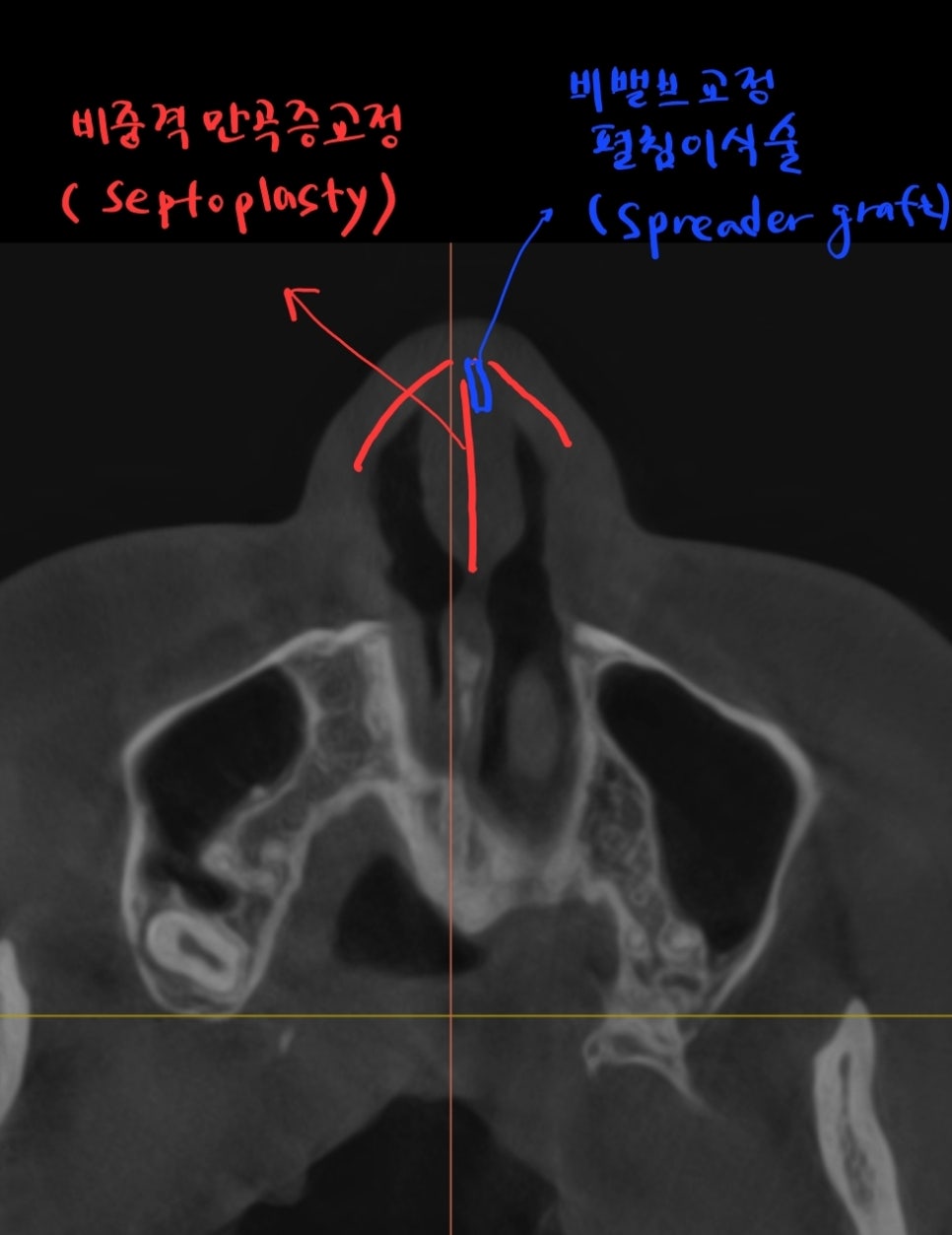
Correction of septal deviation and correction of the obstructed nasal valve
The uneven contour of the nasal bridge caused by saddle nose deformity can be corrected in two ways. First, it can be improved to some extent through the spreader graft mentioned above. The remaining deficiency is usually corrected with a silicone implant.
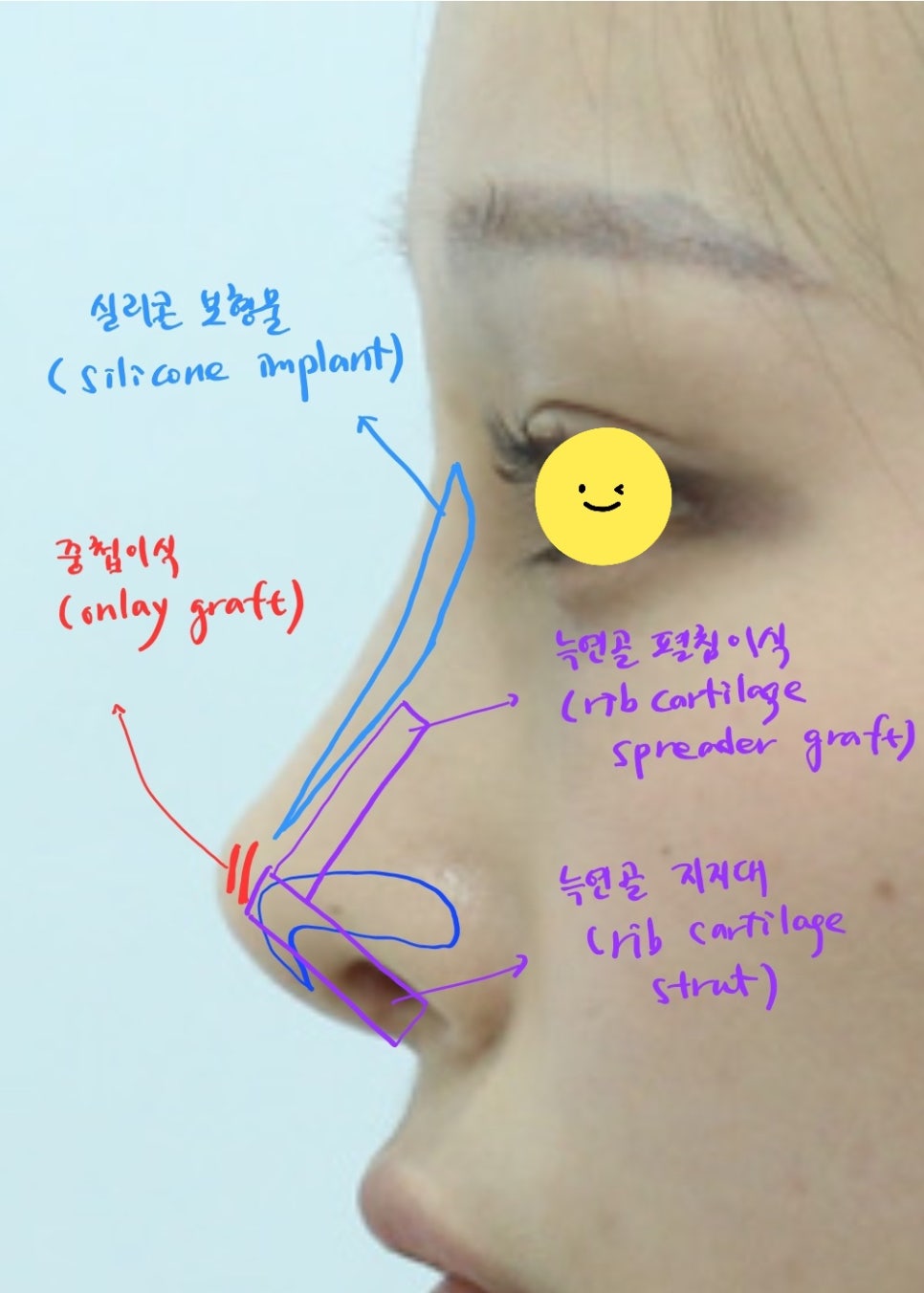
Nasal tip support and silicone implant
To raise the nasal tip, a support structure is built and elevated using rib cartilage, and the nasal bridge is augmented with a silicone implant. To create a point at the nasal tip, a small amount of onlay grafting is used.
The before-and-after results one month after surgery are shown below.
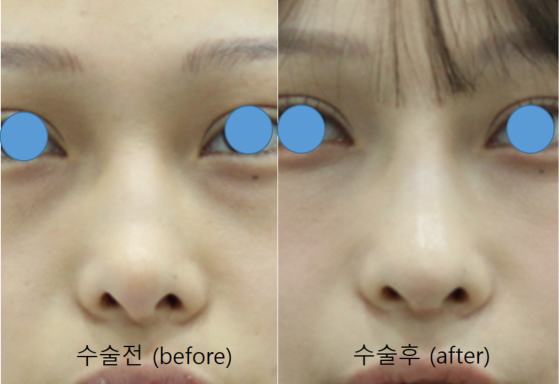
Front view before and after surgery
From the front, the crooked nose and nostril asymmetry have improved greatly.
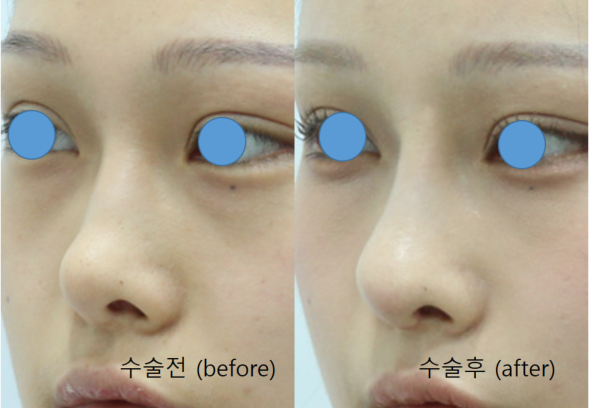
45-degree view before and after surgery
The uneven contour of the nasal bridge before surgery has been improved, giving it a smoother appearance.
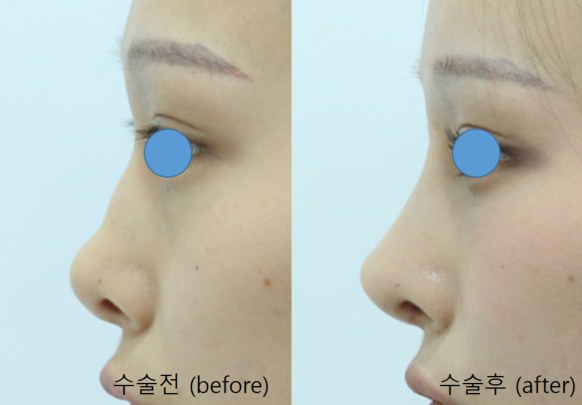
Side view before and after surgery
The bumpy nasal bridge seen before surgery due to the saddle nose deformity has been improved.
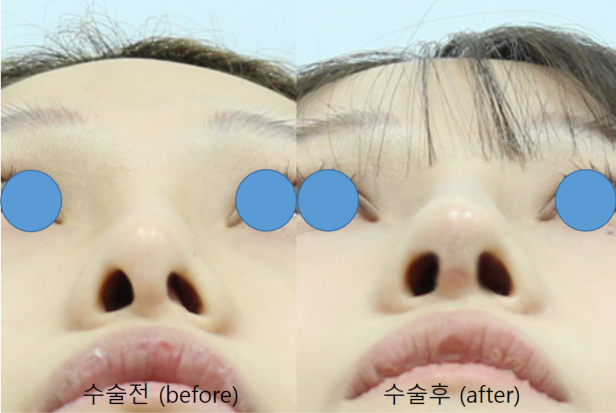
Nostrils before and after surgery
The differences in the size and shape of the left and right nostrils before surgery have improved significantly, and the symptom of the columella collapsing to one side has also improved.
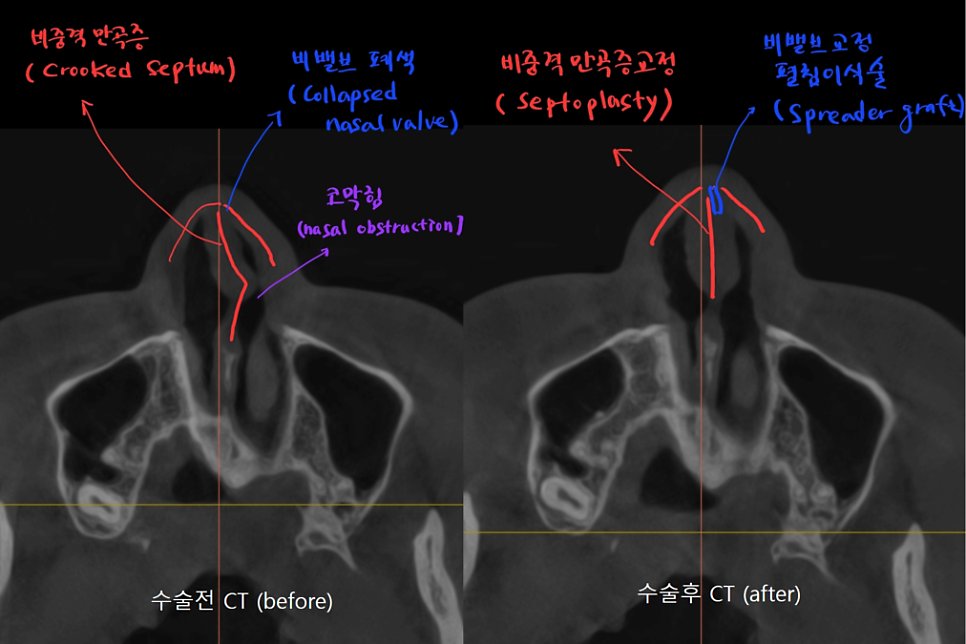
CT before and after surgery
Above all, the biggest improvement is being able to breathe through both nostrils.
The crooked septum inside the nose was straightened, and the blocked nasal valve improved, so the nasal obstruction that caused breathing through only one nostril before surgery was greatly relieved.
When rhinoplasty is performed while improving these functional inconveniences, it can provide satisfaction comparable to the aesthetic satisfaction of having a beautiful nose.
If you do not understand the functional and aesthetic aspects of the nose well, you may think they are unrelated, but the two cannot be considered separately.
A preoperative CT scan can identify problems inside the nose, and if there is septal deviation or nasal valve obstruction, it is best to correct them during rhinoplasty.

This is a real model who consented to disclosure.