In rhinoplasty, the height of the nasal bridge and nasal tip is important, but if we look more closely, the shape of the columella and the angle of the nasolabial angle are also important factors.
'Columella, columella'
The columella refers to the pillar-like part between the nostrils when the nose is viewed from below.
In terms of nasal tip shape, the columella has an aesthetically important relationship with the alae, and the relationship between the columella and the alae can be classified in various ways depending on the shape.
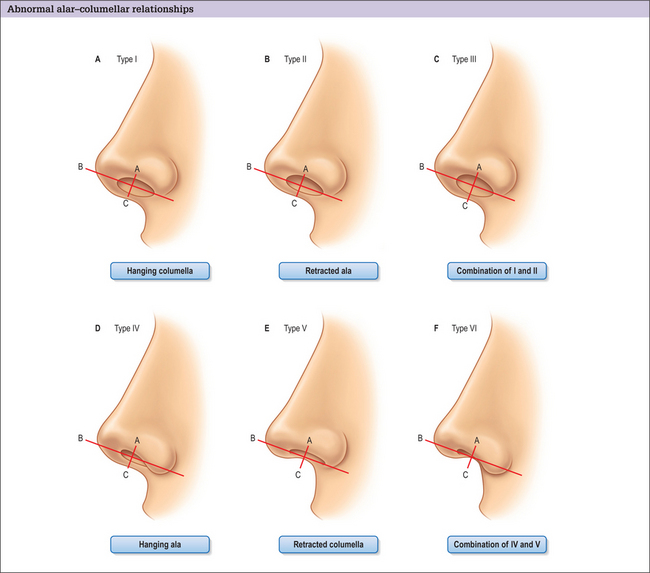
Classification of various shapes according to the relationship between the alae and the columella. (from Plastic Surgery Keys)
'Retracted columella'
When the columella is positioned inward compared with the alae, it is called a retracted columella. It is also often accompanied by sagging alae.

Retracted columella
Especially in people who have had rhinoplasty in the past, the height of the nasal tip may be disappointing, or the columella may not have been corrected, leaving unsatisfactory results in rhinoplasty.
In some cases, inflammation or contracture may make the retracted columella more severe, and in other cases, scars from philtrum reduction surgery may make the retracted columella look more noticeable.

Scar and retracted columella after philtrum reduction
The philtrum and nose are closely related, and many people worry about the order of philtrum reduction surgery and rhinoplasty.
For philtrum reduction surgery, which is performed to make the philtrum look shorter, it is recommended to undergo it after rhinoplasty, because the support of the nasal tip also affects the result of philtrum reduction to some extent.
If you are considering philtrum reduction, it is better to have rhinoplasty that strengthens the nasal tip support using septal cartilage or costal cartilage.
If philtrum reduction surgery is performed before adequate support has been established at the nasal tip, the nasal tip height may decrease and the columella area may appear even more retracted.
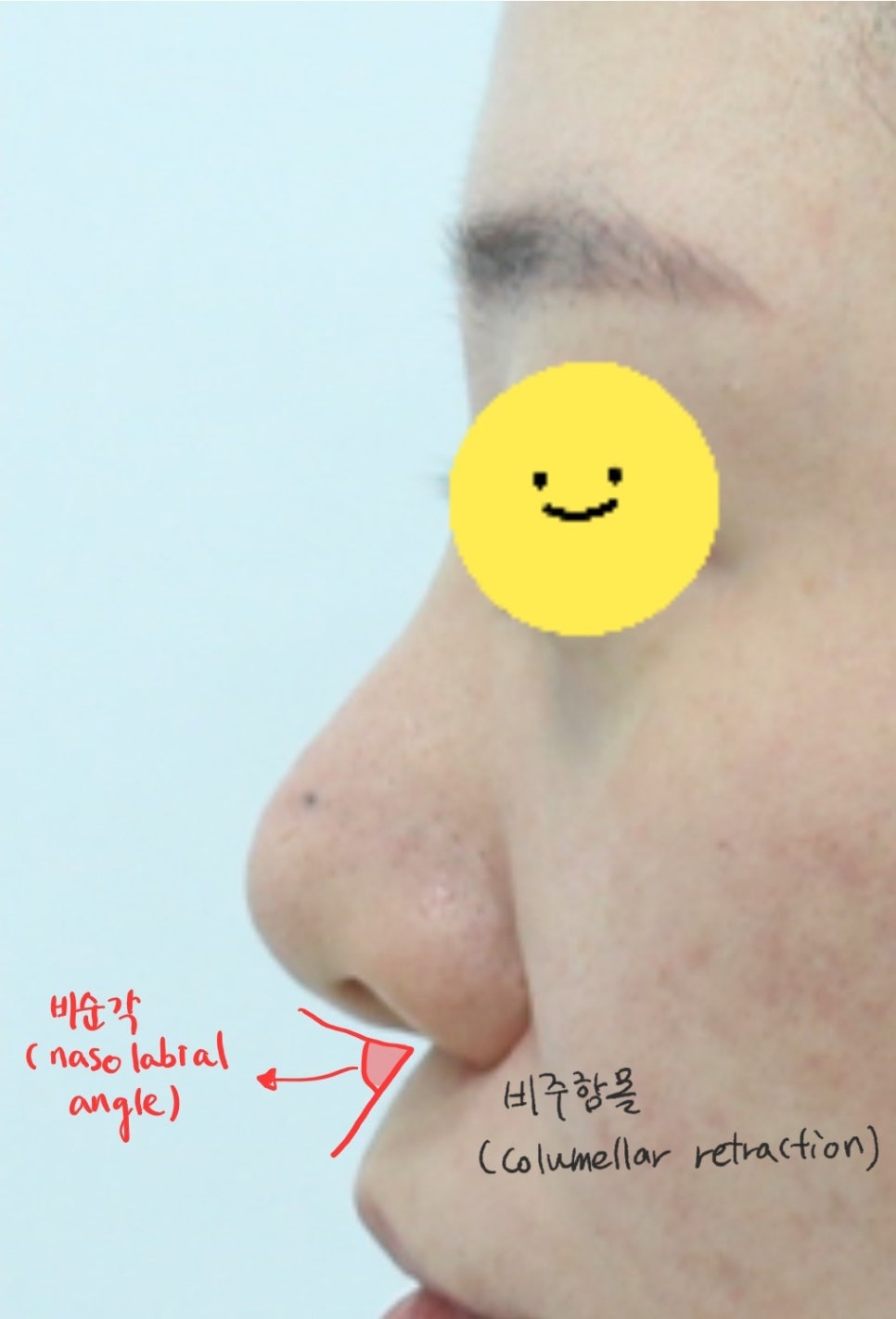
Retracted columella and an acute nasolabial angle
Also, when the columella is retracted and the nasolabial angle becomes acute, less than 90 degrees, the mouth appears protruded, so it does not create a refined impression and the result of rhinoplasty becomes unsatisfactory.
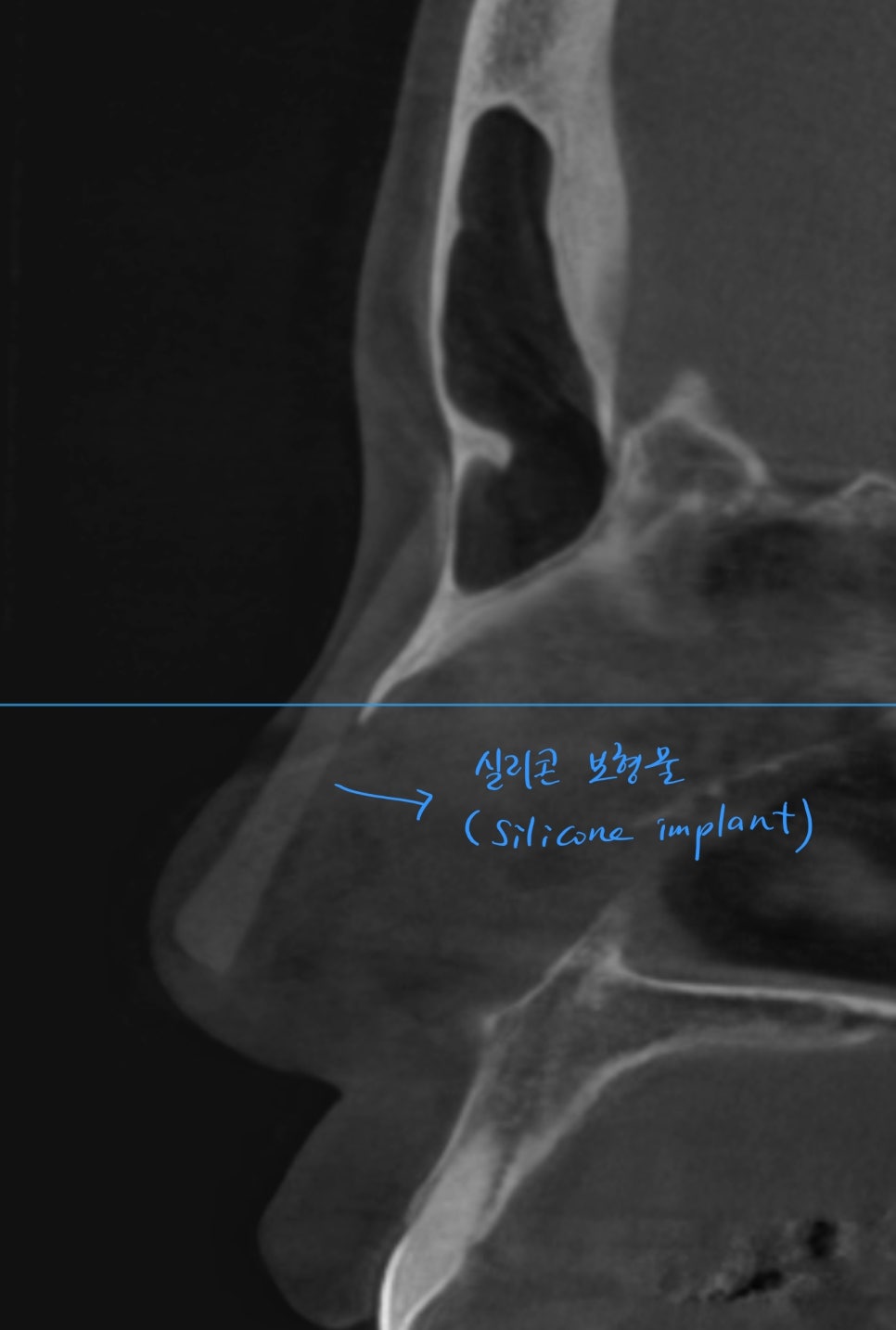
CT scan for consultation for revision rhinoplasty
In the past, silicone implants with a height of 4 to 5 mm were used to raise both the nasal bridge and the nasal tip with silicone.
Because no support structure was created for the nasal tip and the nasal tip was also raised with silicone, good results could not be achieved, and this type of rhinoplasty cannot correct a retracted columella or the nasolabial angle.
'Correction of a retracted columella, lowering the columella, bringing the columella out'
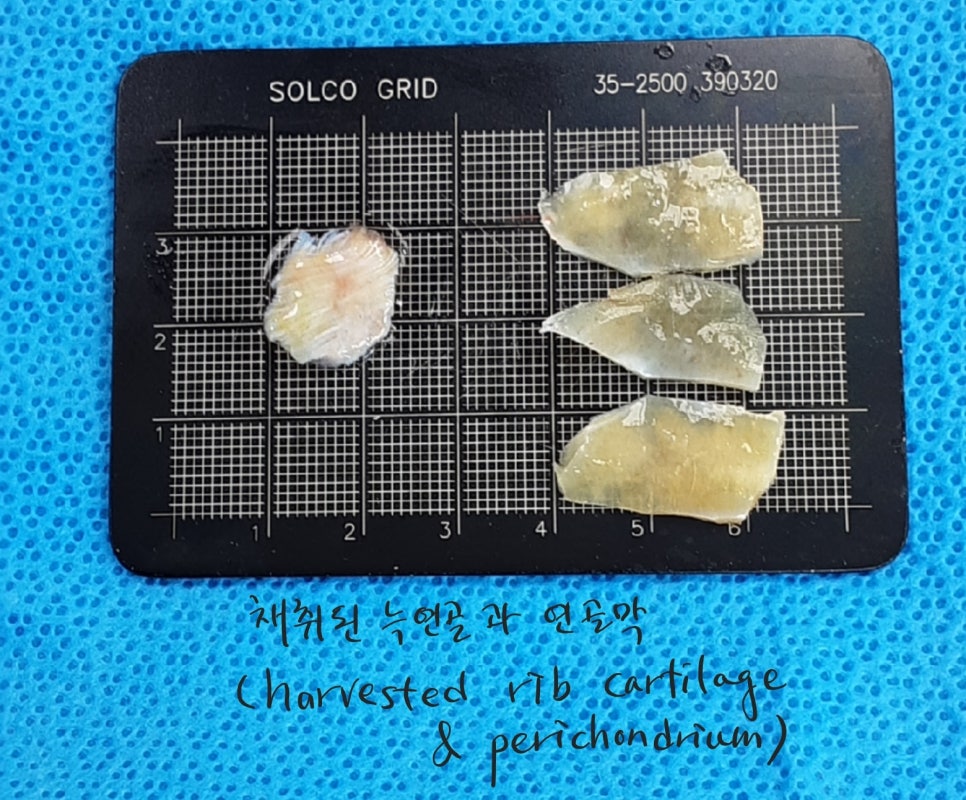
Harvesting autologous costal cartilage for improving a retracted columella and correcting the nasolabial angle
The best rhinoplasty material for correcting a retracted columella and the nasolabial angle is autologous costal cartilage.
Especially when scar tissue from philtrum reduction surgery makes the columella look more retracted, sturdy cartilage material is needed to push up that scar tissue.
After middle age, costal cartilage may become calcified, and the available size of usable costal cartilage may become smaller, but it must be carved into an appropriate shape to secure support for the nasal tip.
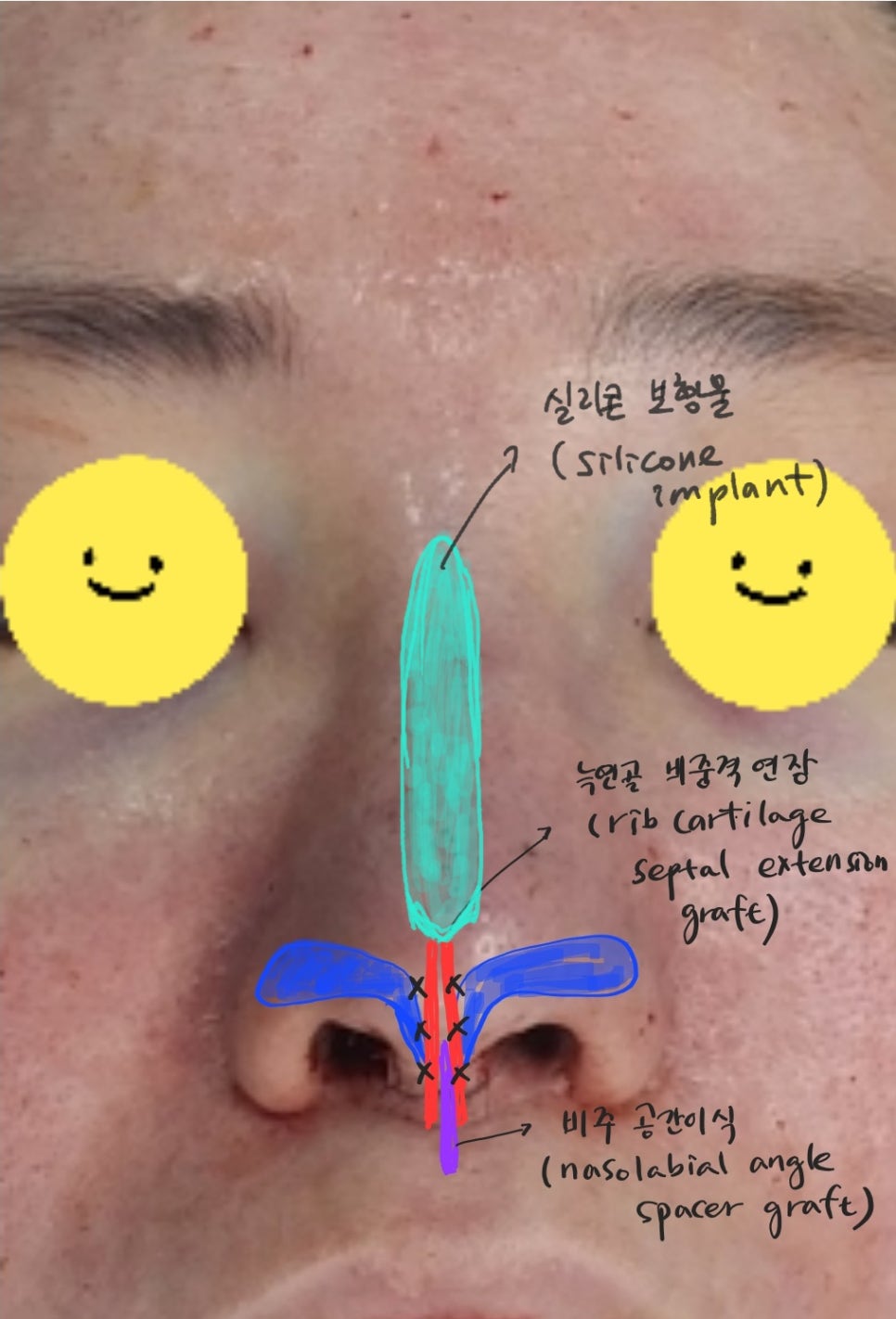
Costal cartilage rhinoplasty for correcting a retracted columella and the nasolabial angle
A septal extension should be created using a piece of costal cartilage between the alar cartilages at the nasal tip, and the septal extension should be performed in a direction that lowers the nasal tip, especially the columella area.
In addition, the adhesions in the scar tissue from the previous philtrum reduction area should be carefully dissected so that the skin can stretch well.
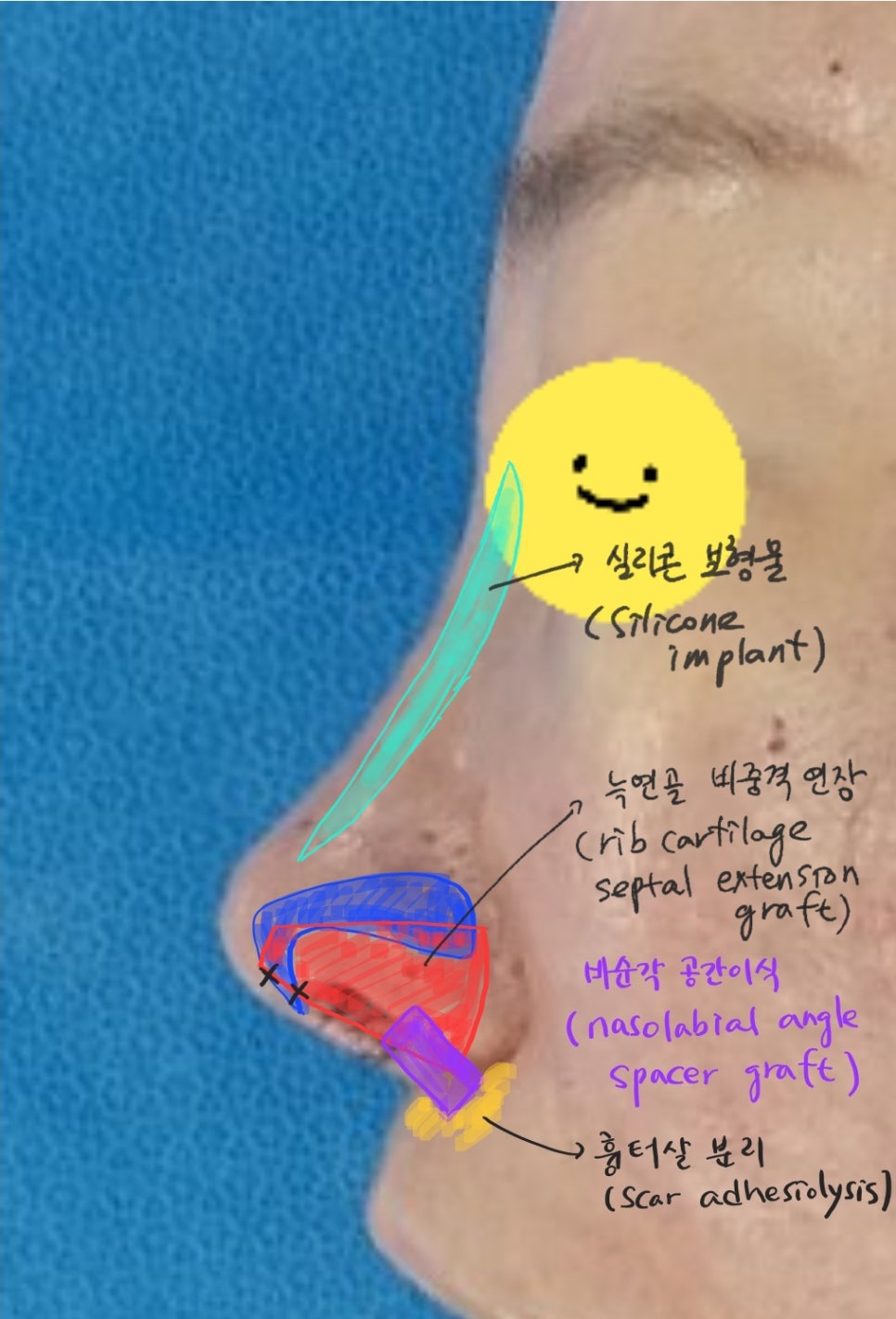
Revision rhinoplasty with costal cartilage for correcting a retracted columella and the nasolabial angle
Using a piece of autologous costal cartilage, the retracted columella area should be brought down well, and after separating the scar tissue in the nasolabial angle area, a piece of costal cartilage should be grafted there again to improve the angle of the nasolabial angle.

Before-and-after comparison of surgery for correcting a retracted columella and the nasolabial angle
Before surgery, the columella was shorter than the alar length, but after rhinoplasty using costal cartilage, the retracted columella was well corrected and lowered to match the length of the alae.

From the side view as well, the retracted columella has come down well, creating a refined shape, and the acute nasolabial angle from before surgery has been corrected to an obtuse angle of over 90 degrees, improving the impression of mouth protrusion.
And because the lowered columella shortens the length of the philtrum, it also shows the effect of philtrum reduction.
To correct a retracted columella or adjust the angle of the nasolabial angle, nasal tip surgery is needed, and the stronger the cartilage supporting the nasal tip, the better the postoperative result.
In the case of philtrum reduction surgery, performing it after sufficient support for the nasal tip has been secured leads to better philtrum reduction results and can also preserve the height of the nasal tip to some extent.