Compared with rhinoplasty in the past, rhinoplasty today has advanced greatly, and thanks to improved surgical techniques, far more detailed methods of nasal surgery have been developed than before.
'Rhinoplasty in the Past'
10 to 20 years ago, rhinoplasty was commonly performed using relatively simple methods, and in particular, it did not sufficiently refine and elevate the tip of the nose.
Past rhinoplasty methods
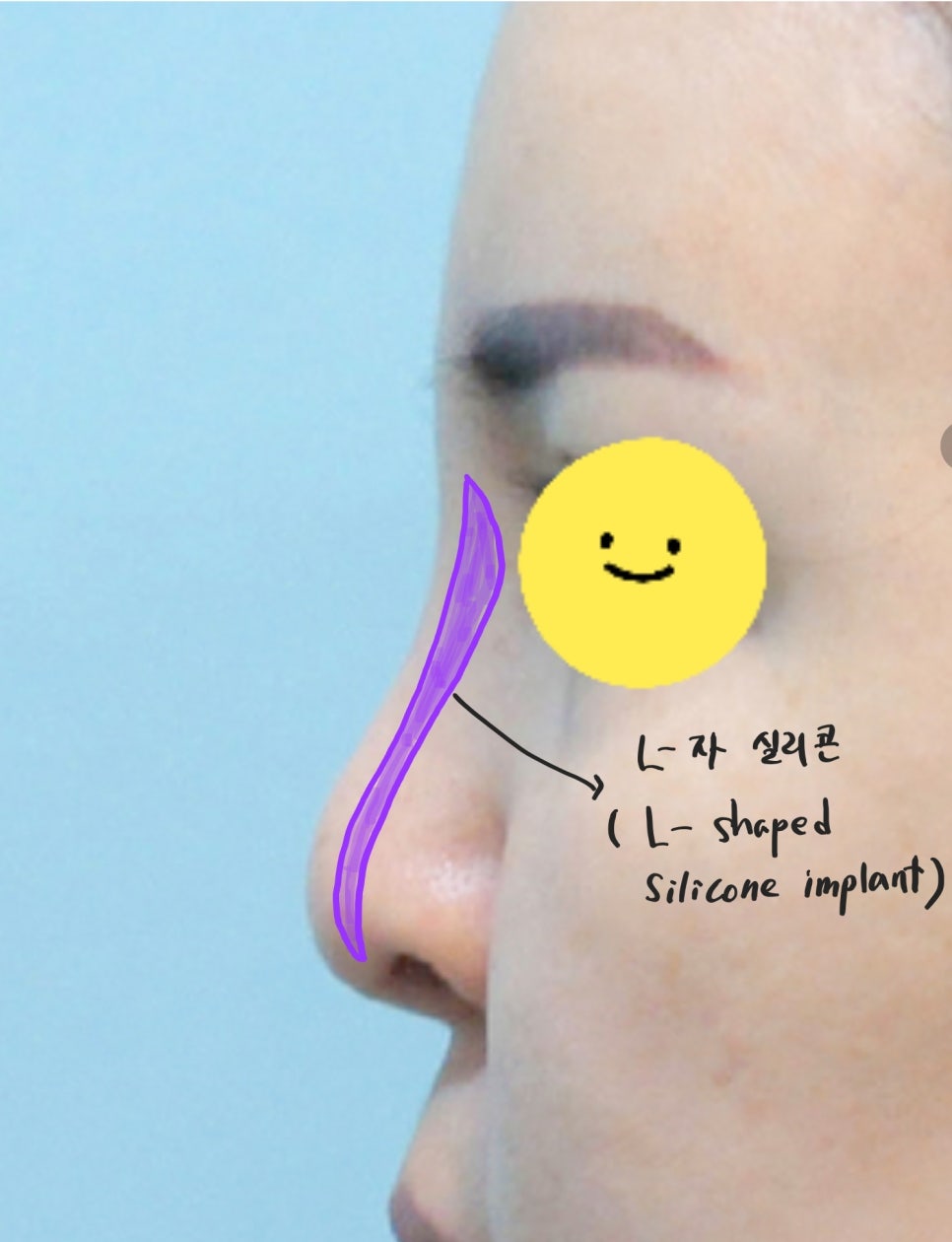
In the past, rhinoplasty using L-shaped silicone implants was also common, and even when I-shaped silicone implants were used, it was common for silicone to be inserted all the way to the tip of the nose.
When asking people who had nose surgery a long time ago about their prior rhinoplasty history, it is common to find that cartilage was not used, or that only something as simple as ear cartilage was used.
To check the silicone implant placed in the past during the preoperative consultation, it can also be confirmed through low-dose CT.
Sometimes, calcification of an old silicone implant can be identified on CT imaging.
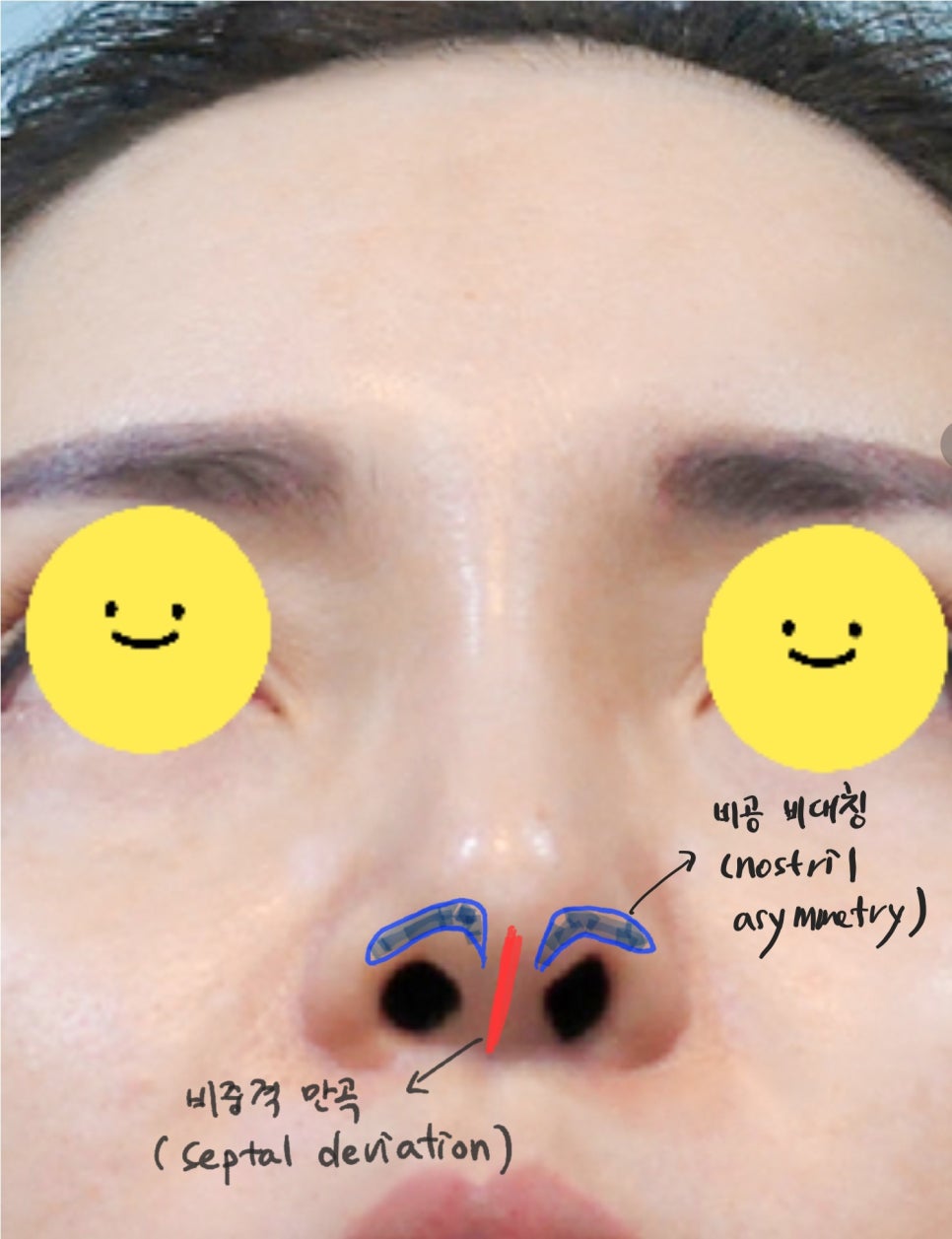
Nostril asymmetry and a deviated septum
And because surgery often involved covering the bridge of the nose all the way to the tip with a silicone implant, there were many cases where fine correction of tip deviation or correction of a deviated septum was hardly performed.
As a result, nostril asymmetry and curvature of the columella often occurred.
'Current Rhinoplasty'
Today, many techniques have been developed that allow the height and length of the nasal tip to be adjusted much more freely, making it possible to sufficiently raise the tip of the nose.
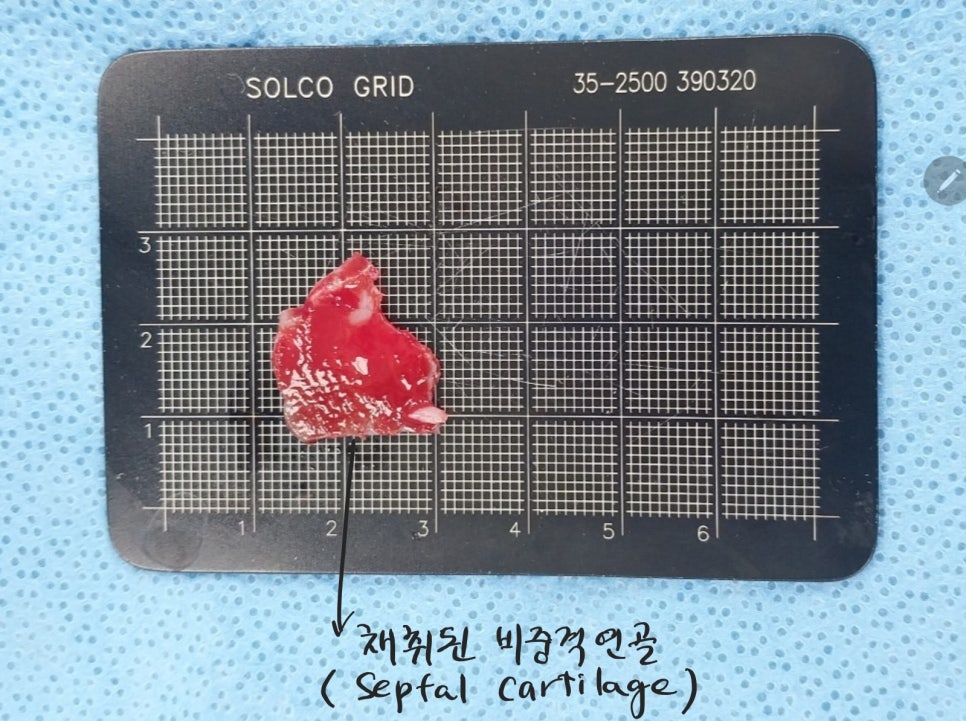
Harvesting septal cartilage for tip surgery
Usually, septal cartilage is mainly harvested to create support for the nasal tip, and if there is insufficient cartilage material, ear cartilage is additionally harvested.
Current rhinoplasty does not connect the bridge of the nose and the tip with a single piece of silicone.
The tip is raised with autologous cartilage material, while the bridge is augmented with I-shaped silicone, so surgery is performed separately for the tip and the bridge.
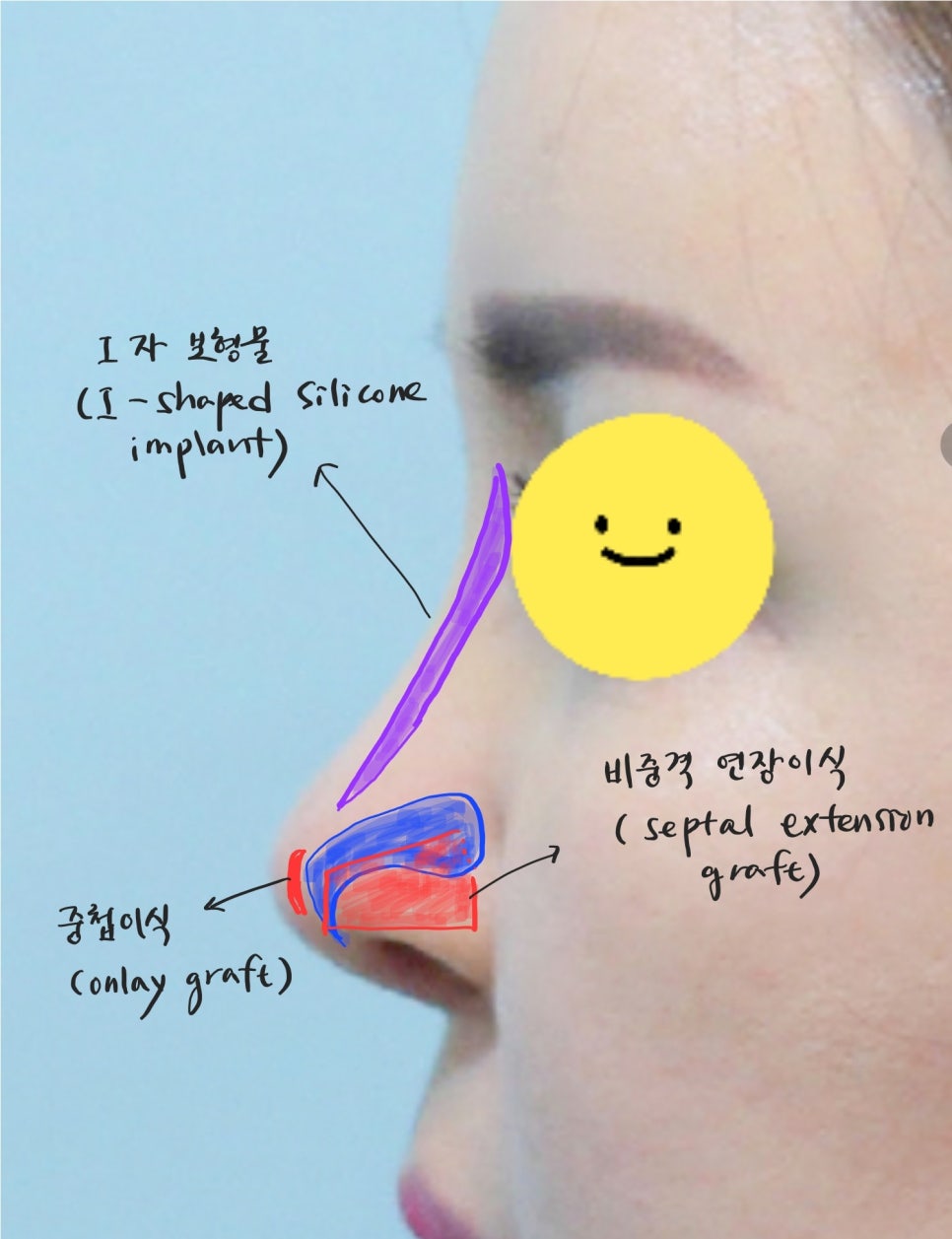
Rhinoplasty using septal extension grafting and I-shaped silicone
For the tip, harvested septal cartilage is extended and grafted onto the existing septum to create support, and if needed, the 부족한 부분 can be raised through overlapping grafting, resulting in a refined nasal tip.
If the nasal tip is short, it can be altered to become longer, and in the case of a long nose with a drooping tip, it can be adjusted in the direction of shortening.
And in the case of L-shaped silicone implants, there are also side effects such as the implant not adhering closely to the bridge of the nose and moving, or causing the skin of the bridge or tip to become thinner. However, I-shaped silicone implants are usually designed to make close contact with the bridge more easily, and surgery is performed so that the silicone implant does not irritate the nasal tip.
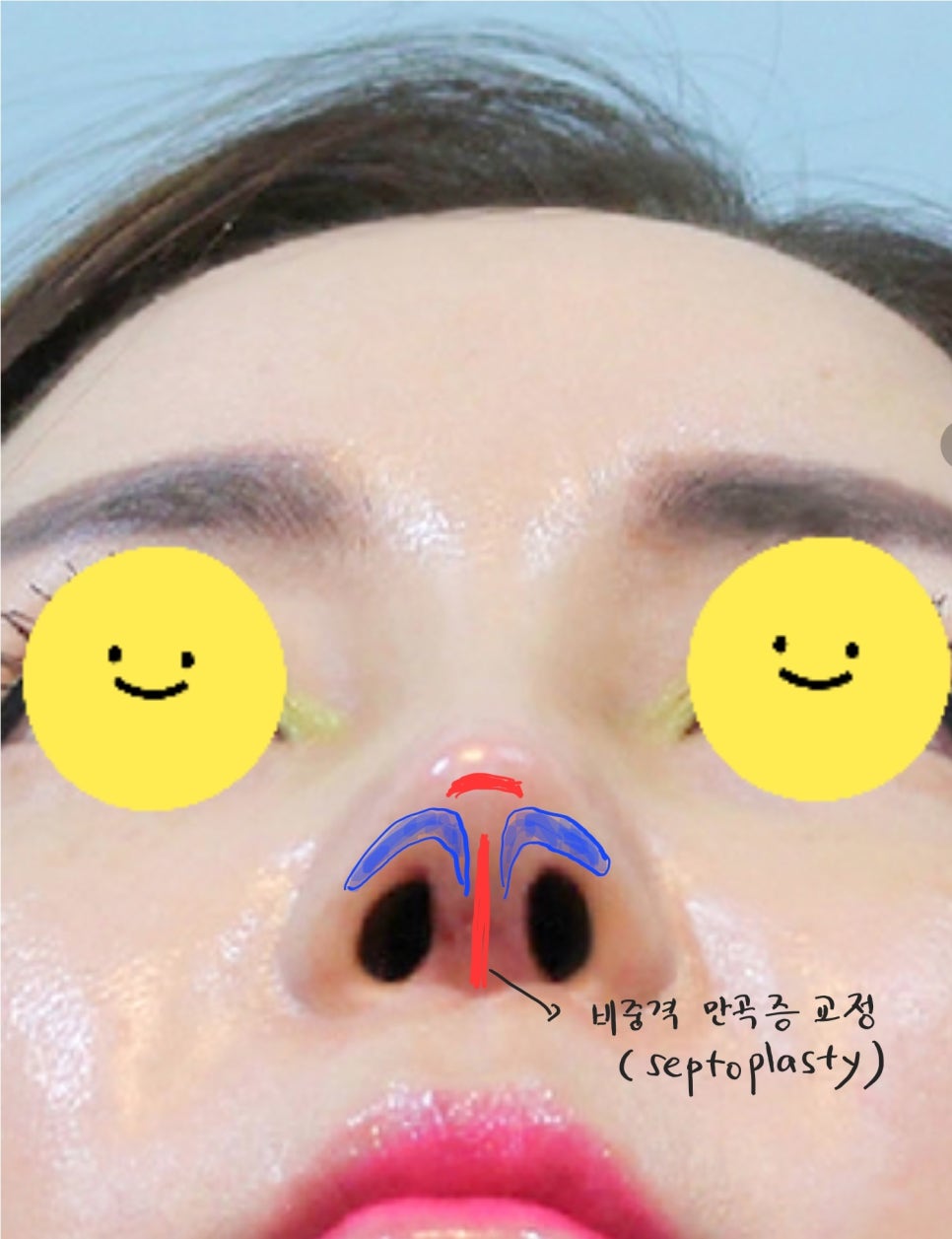
Correction of a deviated septum and correction of nostril asymmetry
Current rhinoplasty actively corrects asymmetry of the nasal tip and a deviated septum.
The height and shape of the nasal tip are important, but rhinoplasty is performed in a way that also delicately corrects asymmetry of the nasal tip and nostrils.
'Middle-Aged Nose Revision Comparison Before and After'
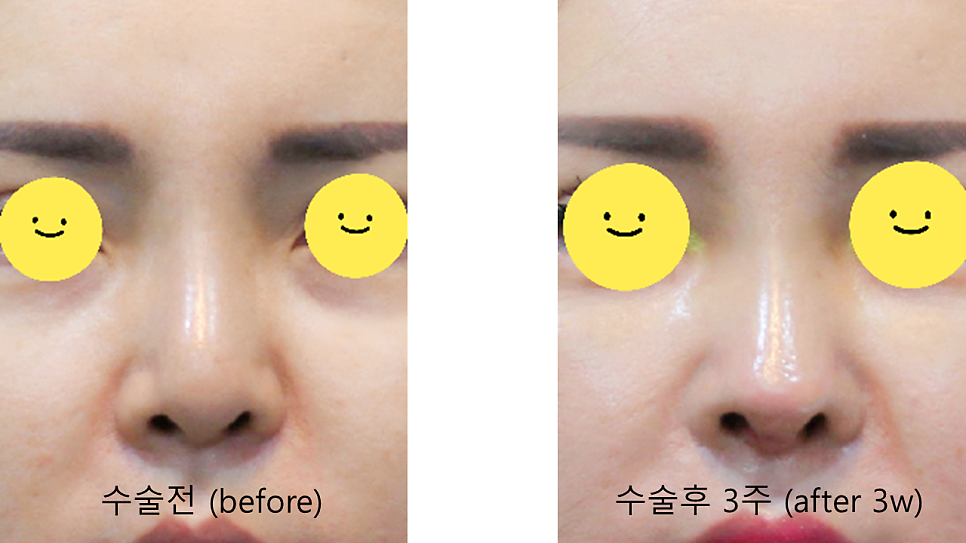
Before-and-after comparison of revision rhinoplasty, front view

Before-and-after comparison of revision rhinoplasty, 45-degree view

Before-and-after comparison of revision rhinoplasty, bottom view

Before-and-after comparison of revision rhinoplasty, side view
Above all, in the past there was a period when the perception of rhinoplasty focused on raising the bridge of the nose, and due to that trend, there were many cases where the bridge became unnaturally high while the nasal tip height was insufficient.
Because this type of rhinoplasty can make the impression look stronger, revision surgery may be needed later in life to achieve a softer appearance.