Hello, I’m Ahn Byung-jun, the chief surgeon at Ahn Byung-jun Plastic Surgery Clinic.
During consultations, some people say, “I was told at another place that my eyes don’t open well, so I was diagnosed with ptosis.”
But when I examine the eye condition directly, there are more cases than you might think where the problem is not with the muscle itself.
It may look like ptosis from the outside, but the actual cause is different. This is called pseudo-ptosis.
If these two are not distinguished and surgery is performed, the desired result may not be achieved, so the diagnostic process is very important.

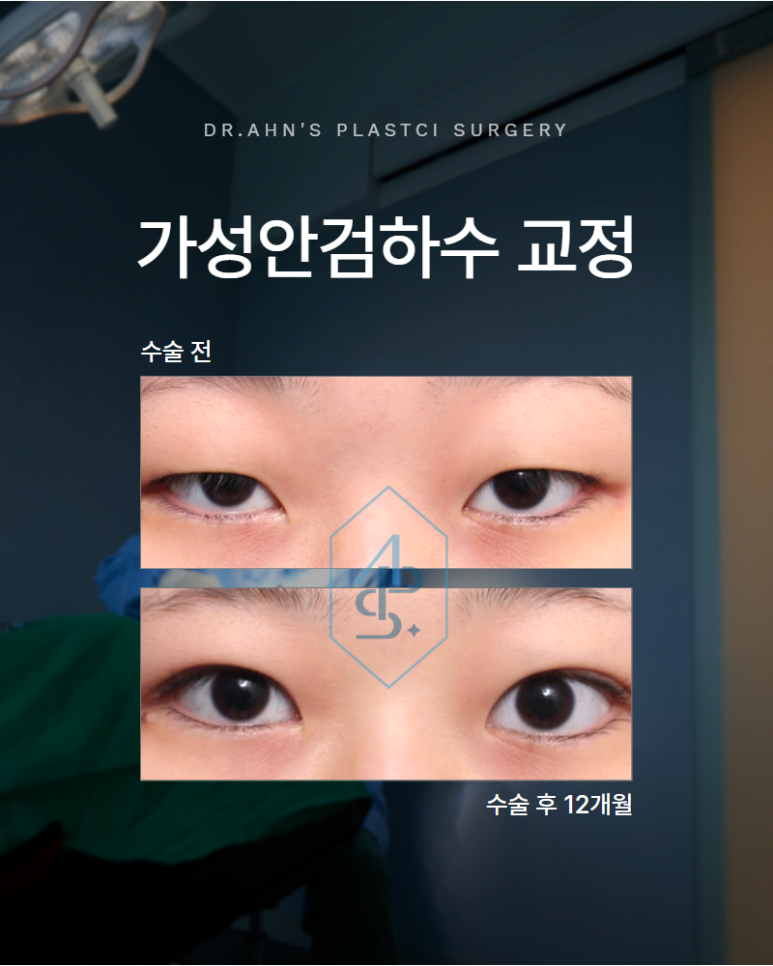
What kind of condition is pseudo-ptosis?
Ptosis is a condition in which the eye does not open fully because the strength of the muscle that opens the eye, the levator muscle or Müller’s muscle, is weakened.
In contrast, pseudo-ptosis is a condition where the muscle strength itself is normal, but the eyelid skin sags, making it look as though the eye opens less.
In particular, eyes that are slightly sunken tend to have eyelid skin covering the black pupil.
In such cases, the pupil does not appear sufficiently from the outside, so it is not easy to distinguish from ptosis.
Just by looking at a photo, it clearly seems like ptosis, but in reality, cases caused by sagging skin fall into this category.
Why is it difficult to distinguish?
There is a reason why it is difficult to distinguish pseudo-ptosis from true ptosis.
In some cases, both conditions are present at the same time.
In other words, the main cause may be sagging skin, while there is also a slight lack of muscle strength.
In such cases, simply addressing the skin is not enough, and it is necessary to determine whether some degree of muscle reinforcement should also be performed.
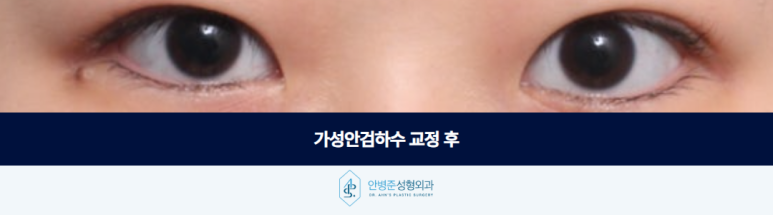
On the other hand, if it is pure pseudo-ptosis with no ptosis at all, then simply correcting the sagging skin can make the eyes open much more naturally.
Therefore, a careful and thorough analysis from multiple angles is needed in advance.
When considering revision surgery after buried-suture or non-incisional eye correction
During treatment, there are patients who come in for revision surgery consultations because they were not satisfied even after having both buried-suture blepharoplasty and non-incisional eye correction.
In many of these cases, surgery was performed after mistaken diagnosis of pseudo-ptosis as ptosis.
The main cause was sagging skin, but because the skin was not addressed and only the muscle strength was reinforced, the eyes became more awkward or led to overcorrection.
These are cases where unnecessary revision surgery could have been avoided if the approach had started with removing the sagging skin.
As these experiences accumulated, I became even more cautious in judging pseudo-ptosis.

How is the surgical direction decided?
When pseudo-ptosis is determined, the basic approach is to remove the sagging skin first.
If the eyes still do not open sufficiently after the skin is corrected, then eye correction surgery is performed only to the extent needed.
Following this order is necessary to prevent overcorrection.
For example, if the line is designed at 8 mm and the surgery is performed by excising 2 mm of skin, a result in which the eyes naturally improve over the course of three months after surgery can be achieved.
It is something we avoid to strongly perform eye correction surgery first and consider the sagging skin later, because that carries the risk of overcorrection or revision surgery.
Pseudo-ptosis is not easy to distinguish by appearance alone.
Before surgery, the structure of the eyes, the degree of sagging, and the condition of the muscles must all be examined together to determine the direction in detail.
If you are concerned that your eyes seem to open poorly, it is important to properly check the cause with an experienced board-certified plastic surgeon.








Previous image
Next image