Hello. I’m Dr. Seo Chan-eol of AB Plastic Surgery.
Today, for those of you considering your first nose surgery because of concerns about your nose, I’d like to briefly introduce primary rhinoplasty and explain the use of a relatively unfamiliar term, “autologous rib cartilage” (hereinafter “autologous rib”).
I hope this will help answer questions such as whether it is really appropriate to use autologous rib cartilage in a first-time nose surgery, what it actually is, and how it is used.
As many people know, “rhinoplasty” is a cosmetic surgery that improves the shape of the nose—an important part of the face—by addressing various concerns such as a nose that is too short or too long, a bridge or tip that is low or drooping, or a nose that is crooked or has a blunt tip.
First, let me explain some commonly used terms in an easy way. There are medical terms for various points of the nose, but in simple terms, the nose can be divided as shown in the image below into the “nasal bridge” (blue arrow) and the “nasal tip” (white arrow). The nasal bridge is the “straight part of the nose,” roughly the upper two-thirds of the nose. The nasal tip is the remaining lower one-third, the highest and roundest part. This area also includes the “columella,” which is the pillar between the nostrils, and the “alar cartilages,” which form the wings of the nostrils.
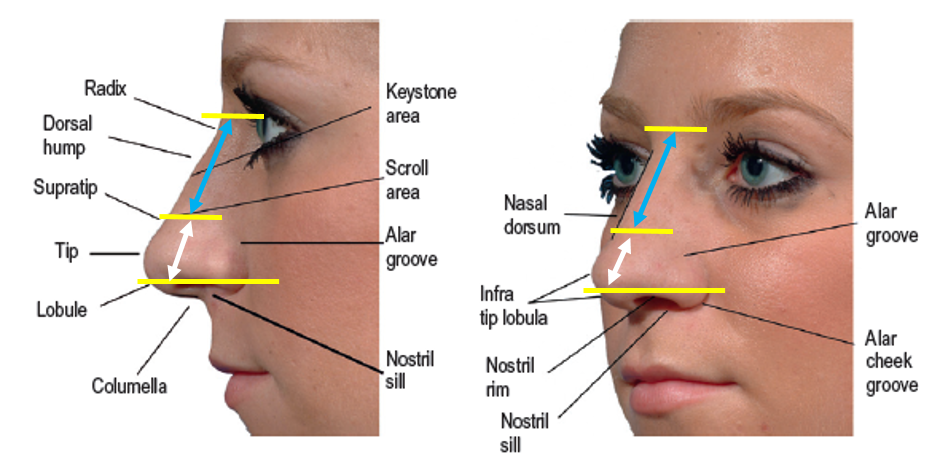
[Figure 1] Components of the nose: nasal bridge (blue arrow), nasal tip (white arrow)
Rhinoplasty basically improves the shape by raising the height of the nasal tip and filling in the line that continues into the nasal bridge with an implant that suits it.
In many rhinoplasty procedures, “autologous rib cartilage” is used as the material to raise the nasal tip, and “silicone” is used as the implant to build up the nasal bridge.
So, let’s look at what “autologous rib cartilage” is, how it is used, whether it is always necessary, and what happens to the area from which it is taken.
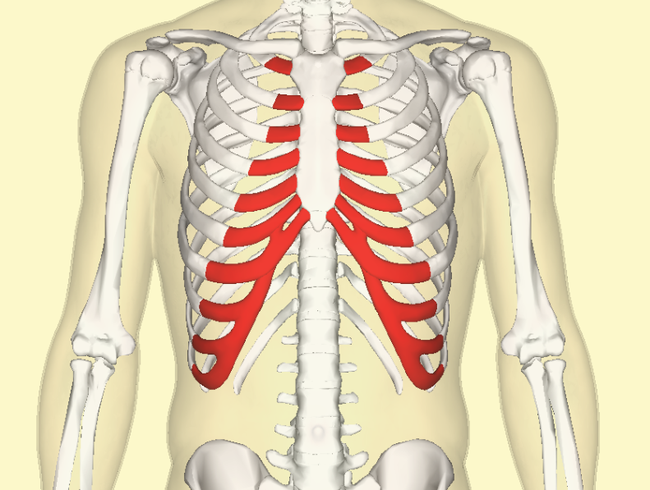
The skeleton that makes up our body and maintains our form consists of “bone” and “cartilage,” which is located between bones and provides flexibility and elasticity. The ribs connect from the waist to the sternum at the front of the chest to protect the organs in the middle of the body, and the front part of the body is made up of relatively flexible and elastic “costal cartilage” (the lower red area).
Previous image
Next image
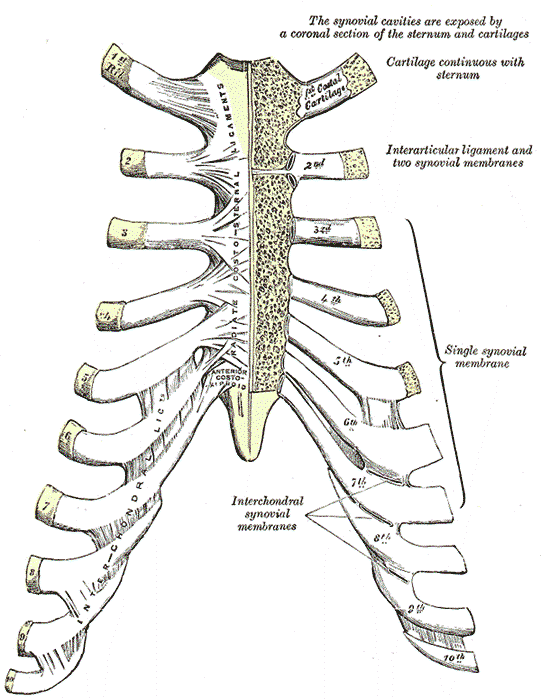
[Figure 2] Ribs and costal cartilage (red markings) [Figure 3] Costal cartilage from 1 to 10
What is commonly called autologous rib cartilage means taking part of your own costal cartilage and using it in nose surgery. To remove it, a horizontal incision of about 2 cm, roughly the length of one finger segment, is made on the skin, and about 3 cm of costal cartilage is harvested from the inside. There are 10 costal cartilages on each side, but a portion of the 7th to 9th costal cartilages is usually harvested so that it can be located in the lower side of the trunk, where the thickness is appropriate and the scar is less visible.
Why costal cartilage, specifically? Compared with other body materials, costal cartilage is firm, long, and has many relatively straight portions, making it suitable for serving as a sturdy pillar that supports the nasal tip. In addition, because there are multiple pieces, there is little functional or aesthetic change even after harvesting.
The harvested costal cartilage is cut crosswise or split in the middle, then fixed in place as a pillar at the nasal tip that needs to be raised.
In the figure below, the existing alar cartilage that formed the low nasal tip is supported and lifted by the raised, sturdy pillar made of costal cartilage (green), changing from the original yellow height to the orange height.
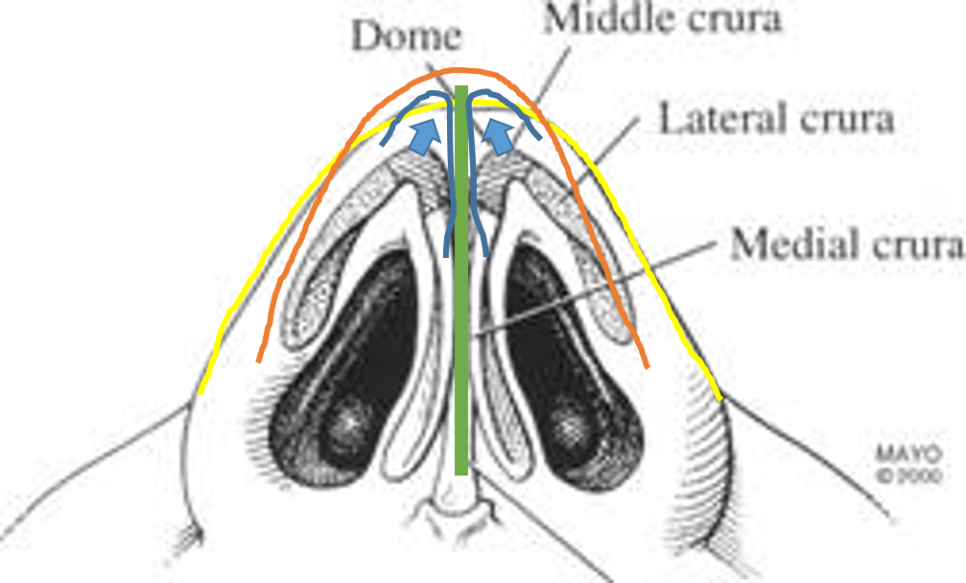
[Figure 4] Costal cartilage pillar (green) and change in nasal tip height (from yellow to orange)
With the nasal tip raised in this way, if the existing nasal bridge is left as is or only partially filled, it becomes a “semi-curved line” that rises toward the end. If the bridge is filled so that it extends in a straight line to match the raised nasal tip, it becomes a “semi-straight or straight line,” as shown by the orange line below.
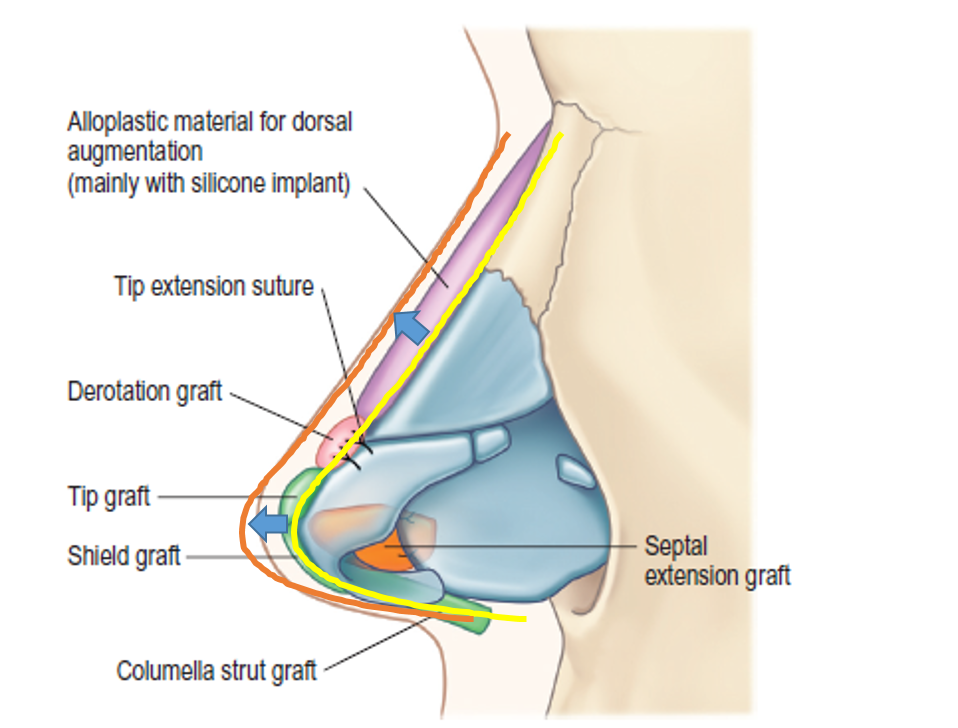
[Figure 5] Changes in the line of the nasal tip and nasal bridge (from yellow line to orange line)
The costal cartilage used in this way is only a portion of the supporting structure that is harvested, and the removed area is gradually filled in with scar tissue over time. Wounds or empty spaces in our body are gradually filled with scar tissue as time passes, and once the space is filled while the surrounding remaining cartilage provides support, the area can remain normal in appearance and function.
So, for a first nose surgery, does one have to use autologous rib cartilage to achieve a high and beautiful nose?
Not necessarily!!
It depends on your own structure (skin thickness, nose shape, nasal bone height, size of the internal cartilage, etc.) and the shape of the nose you want to achieve. Based on these factors, a structure to support the nasal tip may not be needed, or in some cases, ear cartilage or only the septal cartilage inside the nose may be sufficient.
Usually, costal cartilage is considered when the septum inside the nose is crooked, not sturdy, or small, and when a slightly higher and more elaborate result is desired. And even when costal cartilage is needed, if self-harvesting is difficult, donor rib cartilage can be considered.
Today, I focused on giving a brief overview of primary rhinoplasty and the use of autologous rib cartilage. Because nose surgery always involves accurately assessing your original condition and considering the use of cartilage or silicone depending on the desired shape and height, visiting the clinic and consulting with a specialist will be very helpful.
I hope this was helpful in answering the questions you had, and I’ll wrap things up here.