Hello, this is AB Plastic Surgery.
Unlike the nasal bridge, the nasal tip uses only “your own tissue.” In some hospitals, or in the past, materials such as mesh or Medpor were used, but they are now rarely used. Why is that? Unlike the bridge, the nasal tip moves a great deal. It constantly moves with facial expressions. A lot of movement means there can be continuous changes or deformation within the internal tissue as well, and if a foreign material is inserted, it can cause very small internal tissue damage, leading to inflammation or, in severe cases, thinning of the skin and the material breaking through the skin.
The most representative cartilages that can be used for the nasal tip are septal cartilage, ear cartilage, and rib cartilage. I’ll explain the pros and cons of each.
-
Septal cartilage is harvested from inside the nose, so it is easy to obtain and does not leave a scar elsewhere. Also, compared with ear cartilage, septal cartilage is firm, so there is no better material for supporting the nasal tip. Harvesting the septal cartilage is not a new method; in the past, when performing surgery for a deviated septum, the bent portion of the septum was removed, and this is simply an extension of that procedure. In cosmetic surgery, the harvested cartilage is used as the material. In fact, after harvesting, the bent portion of the septum is removed, which can also have a therapeutic effect for a deviated septum. However, in East Asians, it is often relatively small in size. And if the septum is severely bent, you need to be careful because connecting it to a bent septum can make the nose bend even more. It is most accurate to confirm this during surgery, and a preoperative CT scan can show the situation to some extent.
-
Unlike septal cartilage, ear cartilage is soft and flexible. You’ll understand if you touch your ear. When we say ear cartilage, we are not usually harvesting from the part commonly pierced for earrings; instead, we use the concha cartilage inside the ear.
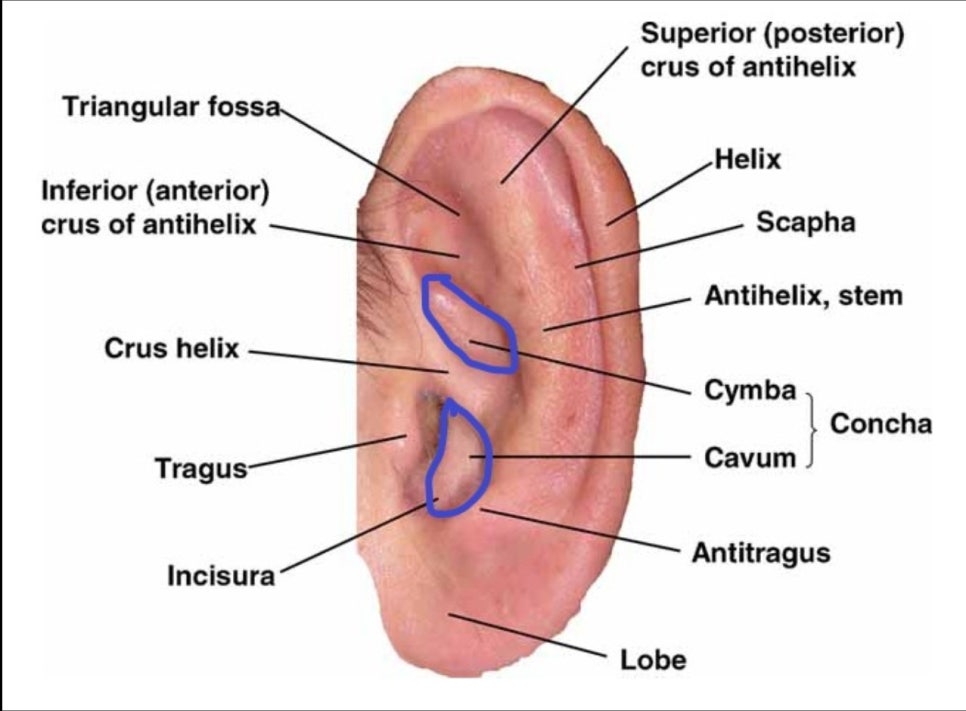
There are two pieces, one upper and one lower, and in my case, I usually harvest the lower one. The reason is that the upper one is longer and can be good in that respect, but in some cases it can cause a slight collapse or deformation of the ear. On the other hand, the lower one is somewhat shorter and thicker than the upper one, but it has the advantage of causing less ear shape deformity. Then is it possible to perform surgery using only ear cartilage without septal cartilage? The answer is yes. However, it is somewhat disadvantageous for short-nose correction. Still, it remains a good material for nasal tip surgery, and because it is softer than septal cartilage, it is good for additional grafting to the nasal tip. When ear cartilage is used alone, it can be a very good material in cases where the patient has undergone previous deviated septum surgery and the septal cartilage cannot be used, and the nasal tip does not need to be raised very much. It is especially useful when the septum is so severely bent that using it for septal extension would make the nose bend even more.
- Next is rib cartilage. In fact, this is the best material. It has all the advantages. It is the strongest and there is plenty of it. It maintains a good shape over the long term. Rib cartilage is generally known to be used in revision surgery, but that is not always the case. In particular, patients with small and short noses often also have small septal cartilage, and as mentioned earlier, ear cartilage is somewhat disadvantageous in short-nose correction, so rib cartilage may be used. When people hear about rib cartilage harvest, they often think it leaves a large scar on the chest and is painful, and the biggest concern is the possibility of pneumothorax. In women, an incision may be made along the inframammary fold, and that scar is usually about 3–4 cm. However, even without doing that, there is a relatively safe way to harvest it with less scarring. Generally, ribs 4–7 are used, but ribs 8 and 9 can be used. The biggest advantage of doing it this way is that the risk of “pneumothorax” is very low.
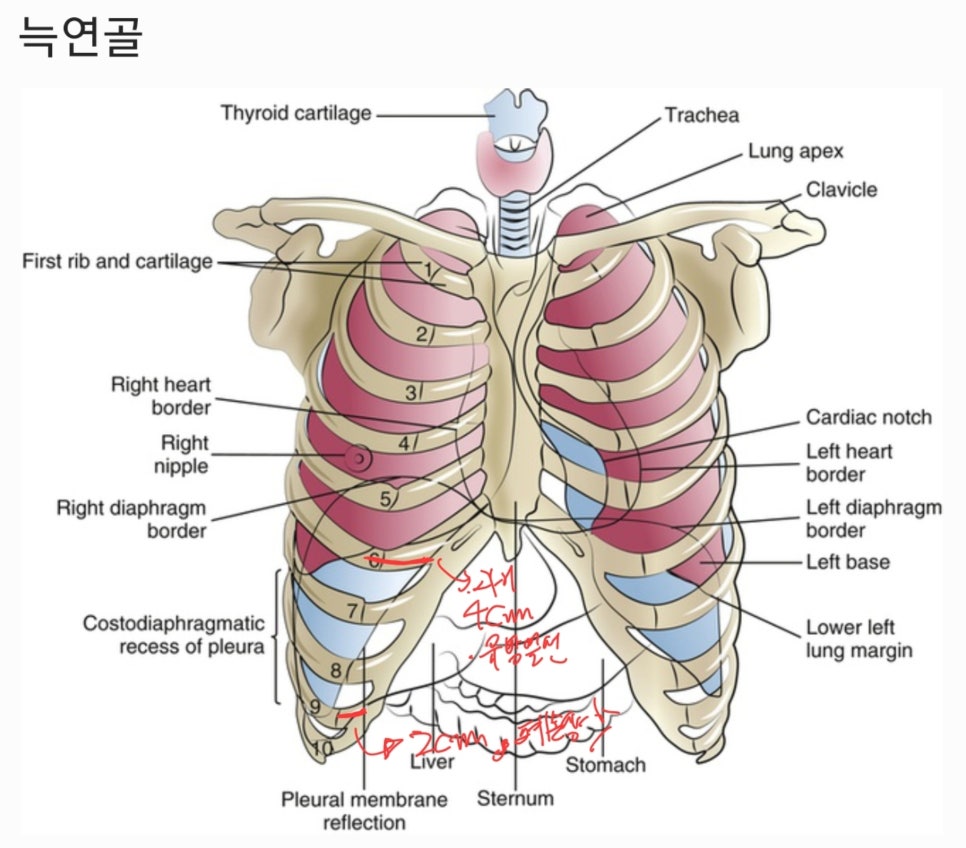
The lungs are located just behind our rib cartilage. The lungs usually extend down to about the 7th rib cartilage, so if cartilage is harvested from the 9th rib, it is far from the lungs, making the possibility of a hole forming in the chest wall, or “pneumothorax,” almost nonexistent. In addition, the scar is about 2 cm smaller, so the pain is also much less. Another concern is that, compared with other cartilages, the nasal tip may move a bit less. There are several factors involved in maintaining nasal tip movement, but usually preserving the membranous septum is important. When performing extension surgery with rib cartilage, if the alar cartilage is completely fixed to the rib cartilage, this membranous septum is lost, and the nasal tip no longer moves. If this membranous septum is preserved, then even when rib cartilage is used, some nasal tip movement can be maintained.
- If the septal cartilage is small or absent due to previous surgery, and ear cartilage is also not suitable, and using rib cartilage feels burdensome, there is an alternative called “donor rib cartilage.” This is processed from dermis donated from a cadaver, similar to donated dermis for the nasal bridge, with the cells removed to eliminate immune reactions. Of course, there is the issue that it can be absorbed more than autologous rib cartilage, but with advances in technology, it is fortunate that even if it is not completely your own tissue, there is still an alternative material for nose surgery.
I hope this answered your question :)
If you have any questions, please leave a comment and I’ll reply.
Thank you!
#NoseSurgery #FirstNoseSurgery #AutologousRibCartilage #RefinedNoseSurgery #RefinedNose #AutologousRibNoseSurgery #SeptalCartilage #EarCartilage #SeptalExtension #ColumellarStrut #DonorRibCartilage