Hello. I’m Dr. Seo Chan-eol from AB Plastic Surgery.
I’ll answer the questions many of you have had about rhinoplasty!
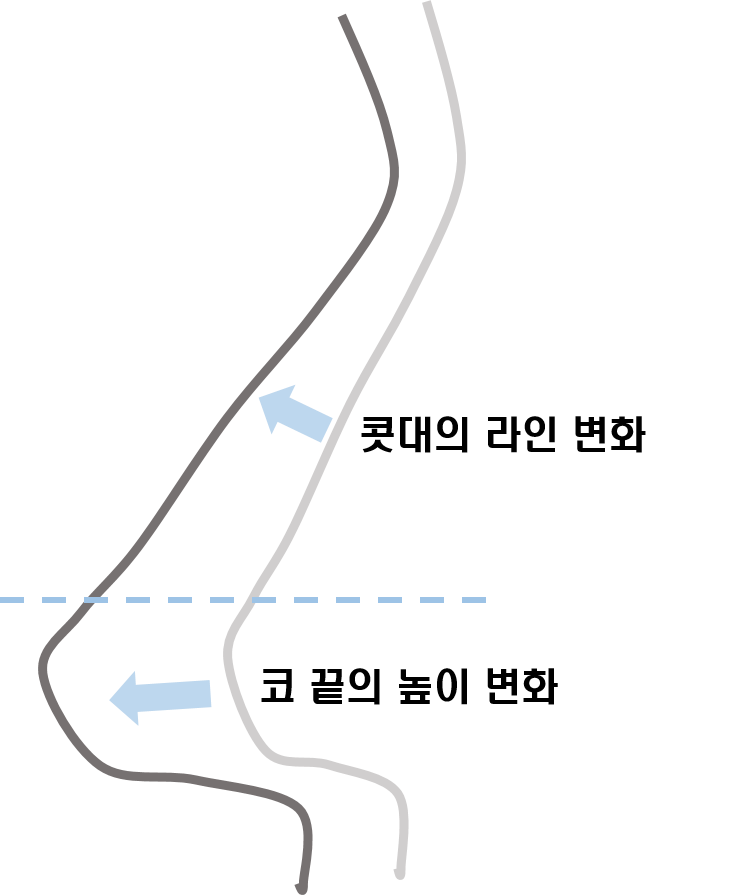
Nose surgery is broadly a procedure that raises the height of the tip of the nose and, according to that raised height, fills in the bridge line.
Recently, most rhinoplasty procedures use “human tissue materials” such as “costal cartilage, ear cartilage, and septal cartilage” to raise the “tip of the nose,”
and use exactly these “implants” or “autologous tissue” to fill in the “bridge line.”
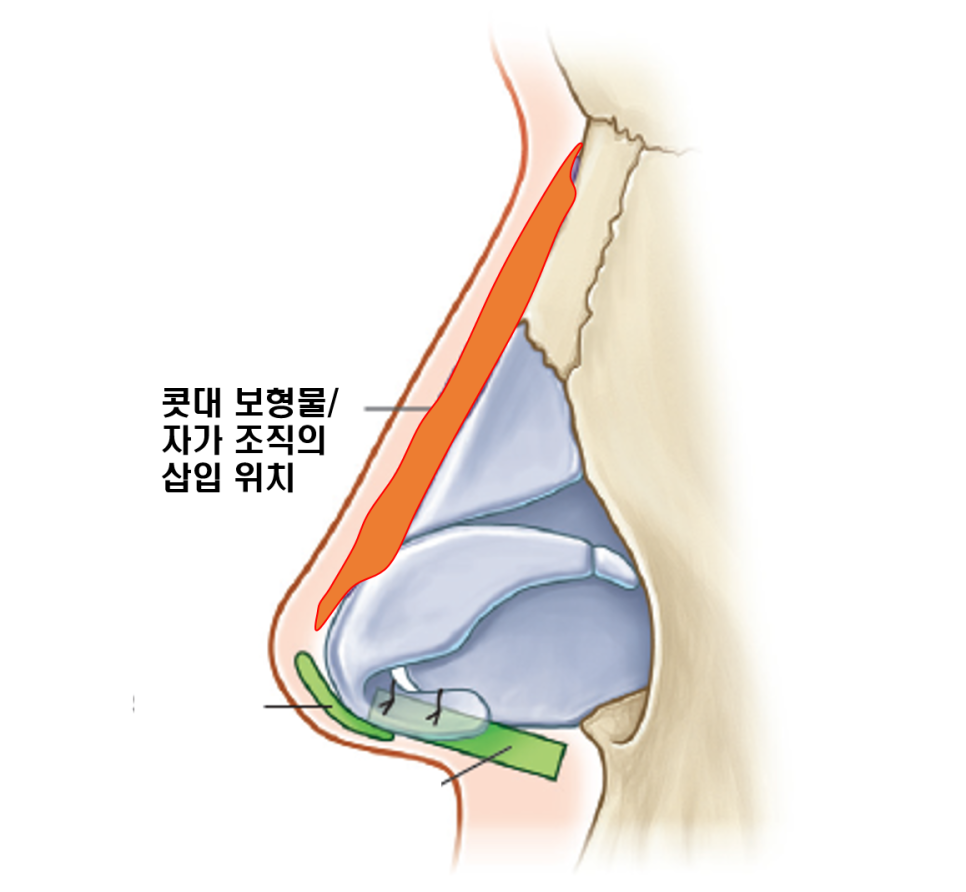
“Implants” are “synthetic materials,” and “autologous tissue” refers to “human tissue materials.” Each has its own advantages and disadvantages, and the right choice is needed depending on the condition and purpose. Today, I’ll explain the implants and autologous tissue that can be used for the nasal bridge, along with their respective pros and cons.
“Implants” mainly use “silicone,” whose safety has been proven over a long period of time, while “autologous tissue” uses “cartilage or dermis” harvested from the human body.
The advantage of implant materials is that they can create a dramatic change in shape, and because they are not reabsorbed, the shape is maintained for a long time. The downside is that, since they are synthetic materials, they are not completely free from inflammation, and in the case of silicone, they can cause contracture deformity over the long term.
Autologous tissue materials have the advantage of being relatively safe in terms of inflammation, but it is difficult to create a dramatic change in shape, and they have the disadvantage that shape maintenance is difficult due to reabsorption.
Shall we take a closer look at when each should be used?
First, let’s look at the most commonly used implant material, the “silicone implant.”
Silicone implants are produced in various shapes and heights, and during surgery, the implant is also modified according to the height differences of the bone to fill in the nasal bridge. Therefore, the biggest advantages are that a large amount can be used to fill the bridge and dramatic changes are possible. In addition, the shape is easy to predict, it is easy to remove if there is a problem, and if there are no issues such as deformation, it can be used semi-permanently. The downside is that, in the long term, there is a possibility of contracture deformity due to the formation of a surrounding capsule.
Another synthetic implant material is Gore-Tex. It was once chosen almost as often as silicone implants, but it was found that it shrinks within the body, reducing its height by 5–20%, which makes it difficult to maintain the shape and hard to predict. Also, unlike silicone implants, it does not form a capsule and tissue grows into the tiny pores on the surface, so if there is a problem, it is difficult to remove. For that reason, its use has greatly decreased in recent years.
Autologous tissue can be classified according to how it is used. There is a method of shaping it like an implant to fill the nasal bridge, and there is another method used when the surgery is only to tidy the bridge line, such as in the case of a hump nose or when the nasal bridge is originally high.
When autologous tissue is made into an implant-like form and used, cartilage itself may be shaved or added on, or the cartilage may be crushed and wrapped in fascia to create an implant-like shape. The advantage is that it is safe in situations where inflammation is mainly caused by synthetic materials, so it can be used by people who feel burdened by the use of synthetic implant materials because of previous inflammation. However, when used in this way, it is difficult to significantly increase the height of the nasal bridge line, making dramatic changes difficult, and partial reabsorption makes changes in shape or height difficult to predict.
However, in cases like a hump nose, where the bridge is originally high and the goal is to improve the tip shape while only filling in the insufficient parts of the bridge to tidy the line, or when someone is seeking only a natural degree of change and feels burdened by implant use, a non-implant surgery that simply fills the bridge line with cartilage is more suitable. I’ll cover this in more detail in another post.
There are also cases that use artificial dermis or autologous dermis. In the case of autologous dermis, the amount that can be harvested is limited and the thickness is not uniform, so while it is suitable for filling in depressed areas of the nasal bridge or for the tip of the nose, it is difficult to use for the entire nasal bridge. In the case of artificial dermis, due to the issue of reabsorption, it is often used as a reinforcement material together with existing materials rather than to fill the nasal bridge by itself.
I hope this was helpful in answering your questions, and I’ll end here.
#ABPlasticSurgery #SeoChanEol #Rhinoplasty #NasalBridgeImplant #Silicone #Dermis #Cartilage