Hello,
This is Kim Tae-young, the chief doctor at Bareunyeong Dental Clinic in Singdang-dong, Yaksu Station.^^
These days, the weather has suddenly gotten hotter,
and perhaps because many people are traveling,
one of the reasons patients come in wanting laminate treatment is,
“When I take photos, I want my teeth to look brighter and prettier.”
“I want laminate because of that reason~”
We often hear this during consultations.
During consultations,
a variety of materials are used, such as facial photos, tooth axis, smile line, and so on.
And sometimes, we find that making a diagnostic model would help with treatment planning a bit more.
When I ask a patient,
“Before starting treatment, it might be more helpful to make a diagnostic model and decide the treatment direction by looking at it.
Would you like us to make one?”
I often get the question,
“Then is a diagnostic model really necessary?”
So today,
I’d like to explain when a diagnostic model is needed for laminate treatment
and whether it is a good idea to make one even for no-prep cases.
What is a diagnostic model??
Simply put, a diagnostic model is a model made by replicating the patient’s tooth condition as it is, and then creating a model of what the final prosthetic result will look like.
In the past, impressions were taken with impression material to make a plaster model, and wax was used to shape it on top of that.
These days, however, using an intraoral scanner to create a digital 3D model can make the result easier to see intuitively.
When is a diagnostic model needed?
The current trend in laminate treatment is
being able to do no-prep laminate when possible,
and, even when tooth reduction is necessary,
reducing only the needed areas by only the necessary amount.
For example, with minimal-prep laminate,
if the teeth are aligned well,
you only need to secure enough space for the laminate overall,
so tooth reduction is done by lightly refining the teeth as a whole.
These days, laminate can be made very thin,
so if some areas cannot be reduced, the restoration can be made with a thinner thickness to compensate.
Cases where a diagnostic model is needed:
- When 기준 for the amount of tooth reduction is needed
- When you want to preview the result after laminate treatment
First, if the alignment or tooth axis deviates significantly from the normal range,
a diagnostic model is needed.
In such cases, of course, a post-treatment simulation can be done, so it is much easier to explain using a diagnostic model.
And because the before-and-after shape can be compared, the patient naturally gains a better understanding of the treatment.
My teeth protrude too much,
so I want them to be brought in.
A patient with front teeth that protruded forward like rabbit teeth wanted them to be brought inward.

Before the diagnostic model
This is the patient’s tooth model before treatment.
The two front central incisors were protruding forward, and the patient came in wanting them to be brought in with laminate.
In cases like this, it is very difficult to decide how much tooth reduction is needed without a diagnostic model, because it is hard to determine how far the teeth should be brought inward in order to create the desired result.

After the diagnostic model
Using a diagnostic model made by predicting the result in advance,
we could see that the teeth could be brought inward to this extent.
If the patient agrees with that, only the necessary amount of tooth reduction can be performed based on the diagnostic model, which helps prevent additional tooth loss.

I want to know if it’s possible without tooth reduction,
and I want to see the result in advance.
Another case
was a patient who wanted laminate treatment for teeth that had rotated, often called “butterfly teeth.”
The patient’s condition was whether this could be done without tooth reduction.
“Butterfly teeth” means that because the teeth are rotated,
the protruding parts need to be brought in to align the teeth,
so those areas have no choice but to be refined.
In cases like this, explaining what I have in my head verbally has limitations,
so since the patient also wanted to try a simulation first, a diagnostic model was performed.
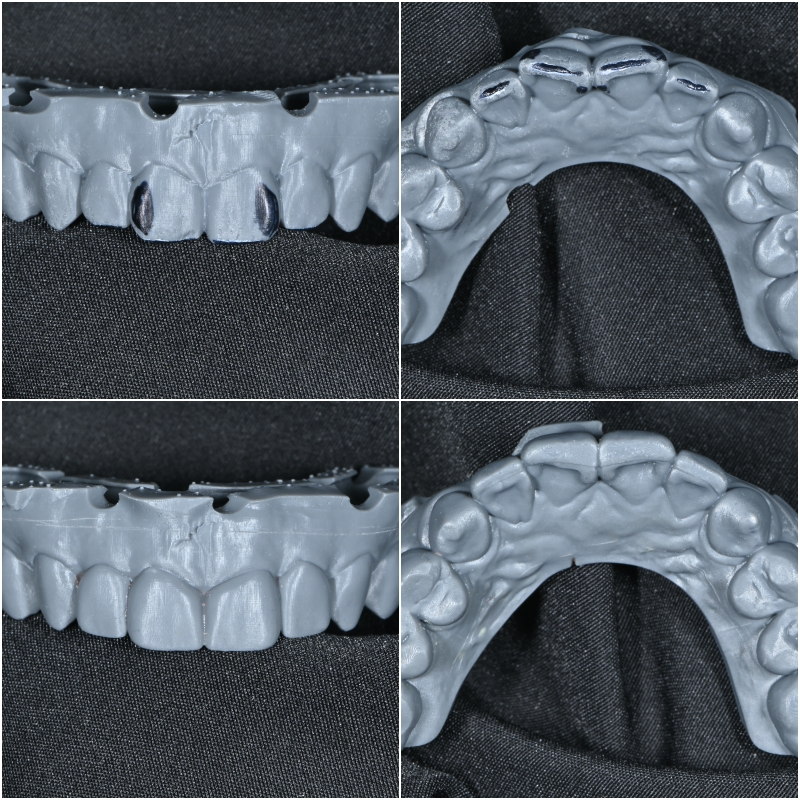
We first analyzed the upper teeth.
The two teeth on top are the patient’s condition before diagnosis.
The two teeth below are the model after the diagnostic result was created.
The diagnosis was that it would be possible if only the sharp protruding parts marked in black on the existing teeth were smoothed.
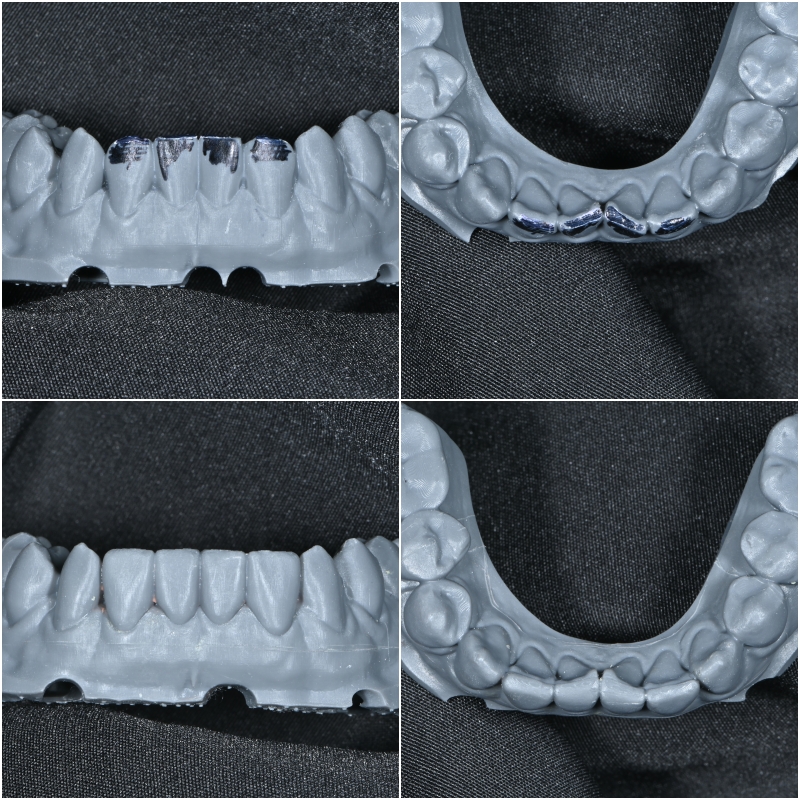
We also analyzed the lower teeth.
The lower teeth are tricky to make without reduction in general,
because they contact the opposing teeth during occlusion.
However, the patient did not want tooth reduction to the point that even if the laminate were removed later, the teeth would still be functional in daily life, so we diagnosed with that in mind.
Fortunately, there was a little space between the upper and lower teeth,
so we decided to use that space.
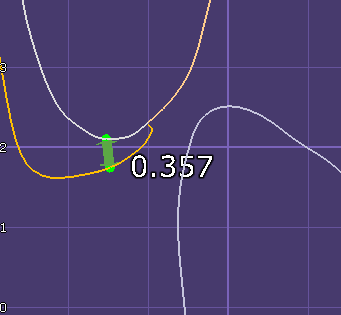
In this way, when the laminate is placed in a space where the upper and lower teeth do not interfere,
we can measure the minimum thickness and secure the necessary thickness.
In this way, through 3D scanning and digital work,
we can understand the before-and-after condition.
I want no-prep laminate,
and I’m curious about how it will turn out.
Second, the reason a diagnostic model is needed is
that I want no-prep laminate without tooth reduction in this current condition,
but I’m wondering whether that would make my mouth look protruded
and what the shape would be like.
No-prep laminate is not always possible,
but it can be limitedly possible for the upper teeth.
However, depending on the existing tooth size, degree of protrusion, tooth shape, and gum shape,
there may be limitations in the tooth shape.
Our mouths are very sensitive.
Even a single strand of hair inside can be felt immediately as uncomfortable.
No matter how thin the laminate is,
it is completely natural to feel awkward at first.
But depending on the degree,
to help the patient decide whether to proceed while taking that into account,
a temporary tooth is made and tried on based on the no-prep laminate diagnostic model.
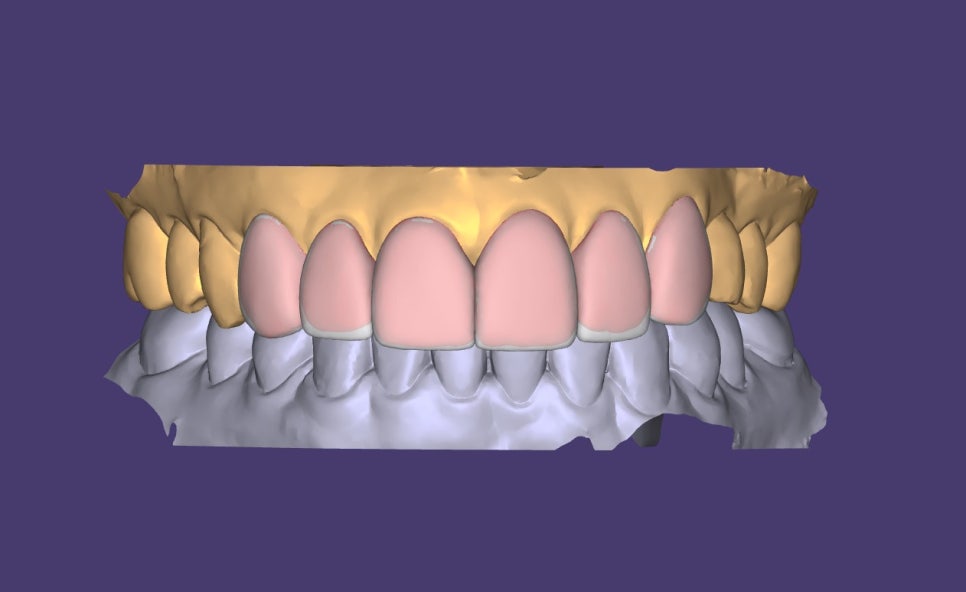
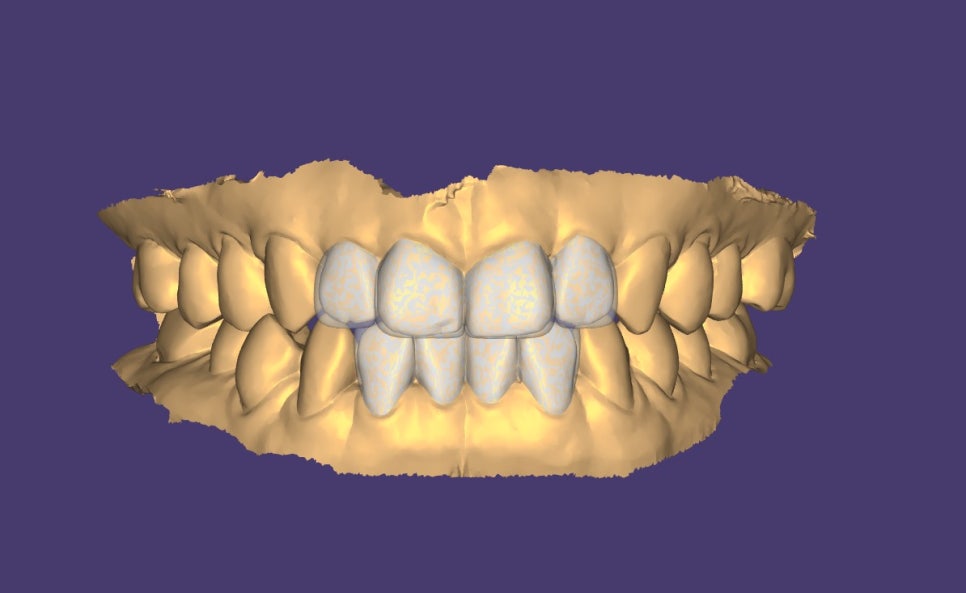
The teeth shown in red are the existing teeth,
and the diagnostic model has been placed over them.
To match the line, short teeth are lengthened,
and the rest are designed with minimal thickness.
At this time, thinner laminate is not always the right answer.
If the patient wants brighter teeth but the existing tooth color is very yellow,
then if the laminate is too thin, the tooth color may show through even if the adhesive is as bright as possible.
So it is necessary to adjust the thickness according to the goal.
Based on this diagnostic model, we can also make a temporary tooth and try it on,
then check how much lip support there is,
whether the tooth shape and size meet the 기준,
and decide whether to proceed with treatment.
A diagnostic model is helpful if you have one,
but it is not always necessary.
However,
it can be essential in some cases
to understand the patient’s needs,
preserve as much tooth structure as possible during treatment,
and reduce teeth efficiently.
That is why,
depending on the patient’s tooth condition,
I recommend discussing it with the medical team and proceeding selectively when needed.
I believe
there is no identical treatment under the same sky.
Even within one person, different teeth have different shapes and characteristics, and because each person has such diverse factors, laminate treatment also looks different depending on the existing tooth shape, facial features, lips, smile, gum shape, and skeletal structure, even if it is made in a similar way.
Therefore, it is necessary to create tooth shapes that suit the patient as much as possible while considering the conditions inside the mouth.
After laminate treatment,
the most common things patients tell me are:
“I can smile naturally when I laugh.”
“I can smile without covering my mouth with my hand now.”
“I didn’t know I could smile like this..”
Since there are people whose impression seems to change,
a natural smile seems to make the overall impression better as well.
Thank you.^^