Hello. I’m Director Jo Hyun-woo of Imtchae Plastic Surgery.
Today, I’d like to talk about Botox procedures, which can be said to be one of the 대표 procedures in recent aesthetic medicine.
Recently, many Botox procedures have been performed.
However, there are also many cases where procedures are carried out without paying close attention to the specific muscle areas and points of action, and many side effect cases have been reported.
So today, I will explain the anatomical locations of the muscles and their mechanisms of action.
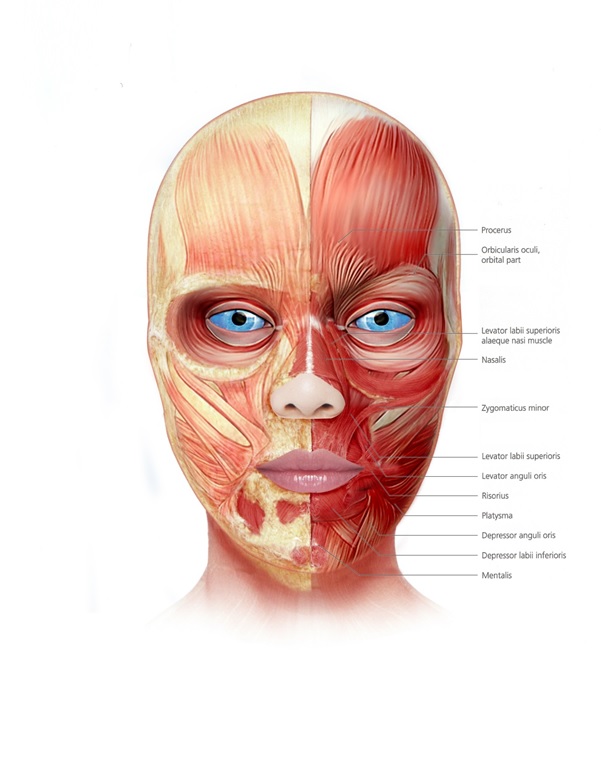
First, the facial muscles you should know for Botox procedures are roughly:
Frontalis muscle, Orbicularis oculi muscle, Corrugator muscle, Procerus muscle, Depressor supercilii muscle, Nasalis muscle, Orbicularis oris muscle, Platysma muscle, and others.
- Frontalis muscle (forehead muscle)
The frontalis muscle originates from the epicranial aponeurosis and blends with fibers of the orbicularis oculi, corrugator, and other muscles before attaching to the skin just above the eyebrows.
When the muscle contracts, it raises the eyebrows and causes horizontal wrinkles on the forehead.
It is also supplied by the temporal branch of the facial nerve.
- Orbicularis oculi muscle (eye muscle)
The orbicularis oculi functions as the sphincter surrounding the eye.
It is divided into three parts: orbital, preseptal, and pretarsal.
The orbital part originates from the nasal part of the frontal bone, the frontal process of the maxilla, and the anterior part of the medial canthal tendon.
These muscle fibers run in an oval shape around the orbit, defining the orbital rim. When the muscle contracts, it can close the eyes tightly, and the upper fibers also depress the eyebrows.
The preseptal part originates from the medial canthal tendon and passes through the fibrous orbital septum to attach to the lateral palpebral raphe.
These fibers help close the eyelids gently.
The pretarsal part begins from the posterior fascia of the lacrimal sac and the crest of the lacrimal bone, then passes laterally to insert into the tarsal plates of both eyelids. These fibers pull the eyelids toward the center and expand the lacrimal sac.
The orbicularis oculi receives innervation from the temporal and zygomatic branches of the facial nerve.
- Corrugator supercilii (eyebrow wrinkle muscle)
It originates from the frontal nasal process just above the medial margin of the orbital rim and extends upward and laterally to attach to the skin just above the center of the eyebrow.
This muscle lies directly over the bone and beneath the frontalis, procerus, and orbicularis oculi muscles.
When the muscle contracts, it depresses the brow, pulls it inferomedially, and creates vertical wrinkles between the eyebrows.
- Depressor supercilii (eyebrow depressor)
It originates from the frontal process of the maxilla, about 1 cm above the medial canthal tendon, has two heads, and attaches to the dermis of the medial brow, playing a role in lowering the eyebrows.
Because it is a thin muscle that is difficult to distinguish from the superomedial fibers of the orbicularis oculi, it must be examined carefully.
- Procerus muscle (nasal muscle, frown muscle)
It originates from the nasal bone and proceeds upward, inserting into the glabella and the dermis between both brows.
It pulls the medial part of the brow downward, creating horizontal wrinkles on the lower forehead and nose.
As will be described later, procedures that use botulinum toxin to block the action of the procerus and corrugator to reduce frown lines are very common, and in endoscopic forehead lifting, procedures to reduce the procerus are also sometimes performed.
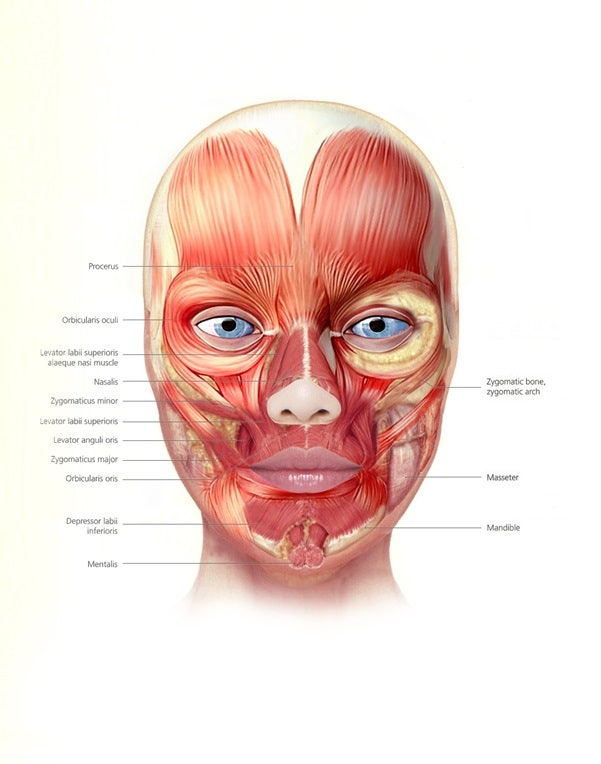
- Zygomaticus major & minor (major and minor zygomatic muscles)
As superficial muscles, they originate from the body of the zygoma and run downward to insert at the corner of the mouth and the lateral border of the upper lip.
They receive innervation from the zygomatic and buccal branches of the facial nerve and play a role in lifting the corners of the mouth.
- Levator labii (upper lip elevator)
This muscle lies below the orbicularis oculi and originates just above the infraorbital foramen.
It runs downward and inserts into the upper lip and orbicularis oris. The levator labii superioris alaeque nasi, located along its medial border, begins at the frontal process of the maxilla and attaches to the nasal cartilage and upper lip.
These two muscles receive innervation from the buccal and zygomatic branches of the facial nerve and help lift the corners of the mouth.
- Levator anguli oris (corner of mouth elevator)
It originates from the canine fossa below the infraorbital foramen and attaches to the upper lip.
It receives innervation from the buccal and zygomatic branches of the facial nerve and helps lift the corners of the mouth.
- Risorius (smile muscle, corner-of-mouth retractor)
The risorius is often underdeveloped and arises from a thickened part of the lateral cheek platysma, attaching to the corner of the mouth.
It pulls the mouth laterally.
- Orbicularis oris (mouth muscle, lip muscle)
It functions as a sphincter surrounding the mouth, and its muscle fibers are connected with all the other facial muscles that act on the mouth.
It is influenced by the buccal and marginal mandibular branches of the facial nerve and plays a role in puckering, widening, and closing the lips.
- Depressor anguli oris (corner-of-mouth depressor)
It originates from the periosteum of the oblique line of the mandible, lateral to the depressor labii inferioris.
This muscle merges with the orbicularis oris, risorius, and levator anguli oris to form the modiolus. It receives innervation from the marginal mandibular branch of the facial nerve and, when contracted, lowers the corners of the mouth.
- Depressor labii inferioris (lower lip depressor)
It originates from the oblique line of the mandible in front of the mental foramen, covering the depressor anguli oris, and runs upward and medially to insert into the skin and mucosa of the lower lip and the fibers of the orbicularis oris.
- Mentalis (chin muscle)
It originates from the incisive fossa of the mandible and runs downward to attach to the dermis of the chin.
When it contracts, it lifts the lower lip and projects it forward, creating dimpling of the chin skin, which is called a peach pit.
It is supplied by the mental nerve.
- Nasalis (nose muscle)
The nasalis is divided into the transverse part (compressor naris) and the alar part (dilator naris). The compressor naris begins at the canine tooth area of the maxilla and attaches to the opposite muscle on the dorsum of the nose. It compresses the shape of the nose. The dilator naris originates from the axilla of the medial lower part of the compressor naris and attaches to the alar cartilage of the nose. It helps widen the nostrils during breathing.
The depressor septi originates from the maxilla above the central incisor and the upper lip from the mucous membrane, then inserts into the cartilaginous nasal septum and pulls the nasal tip downward. All of the above muscles are supplied by the upper buccal branch of the facial nerve.
- Platysma (neck muscle)
It is a thin muscle originating from the fascia of the chest and shoulder muscles and extending from the clavicle toward the lower face and neck.
It attaches to the lower border of the mandible, the muscles around the mouth, the modiolus, and the dermis of the cheek. As people age, the medial muscle fibers become more bundled and thickened, forming platysmal bands. Functionally, the platysma lowers the mandible during deep breathing, is regarded as a downward extension of the SMAS, and receives innervation from the cervical branch of the facial nerve.
- Masseter (chewing muscle)
In addition to softening facial wrinkles using botulinum toxin, procedures that reduce the volume of the masseter using toxin have also been performed frequently in recent years. The masseter is a rectangular, thick, and powerful chewing muscle.
The superficial part originates from the zygomatic process of the maxilla and the anterior two-thirds of the lower portion of the zygomatic arch, then descends downward and backward to insert into the lower half of the lateral surface of the angle and ramus of the mandible.
The deep part originates from the medial side of the zygomatic arch, descends, and inserts into the upper portion of the ramus and the lateral surface of the coronoid process. It is innervated by the mandibular branch of the trigeminal nerve.
So far, I have described the various muscles involved in facial expression and mastication.
I hope this has been helpful for Botox procedures by referring to the actions and locations of the muscles described above.
Thank you.
zygoma reduction surgery, square jaw reduction surgery, cortical ostectomy, chin reduction surgery

zygoma reduction surgery, square jaw reduction surgery, cortical ostectomy, masseter resection surgery