Hello, this is Director Jo Hyun-woo of 3D Plastic Surgery.
Today, I’d like to explain a possible complication after zygoma surgery, called nonunion, along with real cases.
During consultations and while reviewing post-surgery progress, many people worry about nonunion.
In zygoma surgery, nonunion refers to the cut zygomatic bones not joining together.
What many of you may be overlooking is that a more serious complication than cheek sagging is nonunion.
If nonunion occurs, cheek sagging will naturally follow.
As a result of nonunion, the patient not only experiences cheek sagging but also pain at the area where the bone has not joined, and may feel the bone moving when chewing food.
Why does nonunion happen?
Causes of nonunion can include fixation problems, surgical issues, or the patient’s carelessness.
It can occur when fixation was not done properly, was not done at all, or when a fixation pin breaks.
In cases of incorrect surgery, nonunion can occur regardless of whether fixation was done, so caution is needed.
To prevent nonunion after zygoma surgery, you should limit strenuous chewing for about 6 weeks.
If the surgery was performed correctly, then as long as you avoid excessively chewing tough or hard foods while the bone is healing, you can confirm with a CT scan 6 weeks after surgery that the bone has joined well.
Therefore, if the surgery was done properly, nonunion is very rare as long as you are careful during the bone-healing period, and it can be sufficiently prevented through the medical team’s careful management during and after surgery.
This is where real patients start to have questions.
When I see patients coming in for revision zygoma surgery consultations, they often say, “I had a CT scan at another hospital, and it showed nonunion.”
So when we take a CT scan,
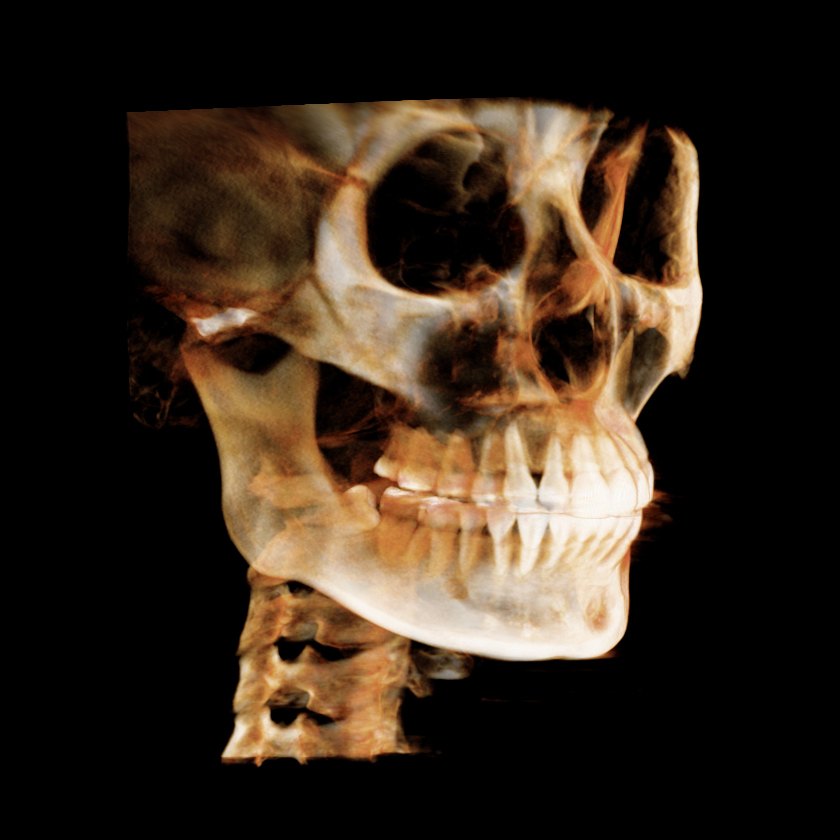
they point to the dark-looking area in the photo above and say the bone has separated, the surgery was done incorrectly, it’s nonunion, and revision surgery is needed.
But if you change the shading a little,
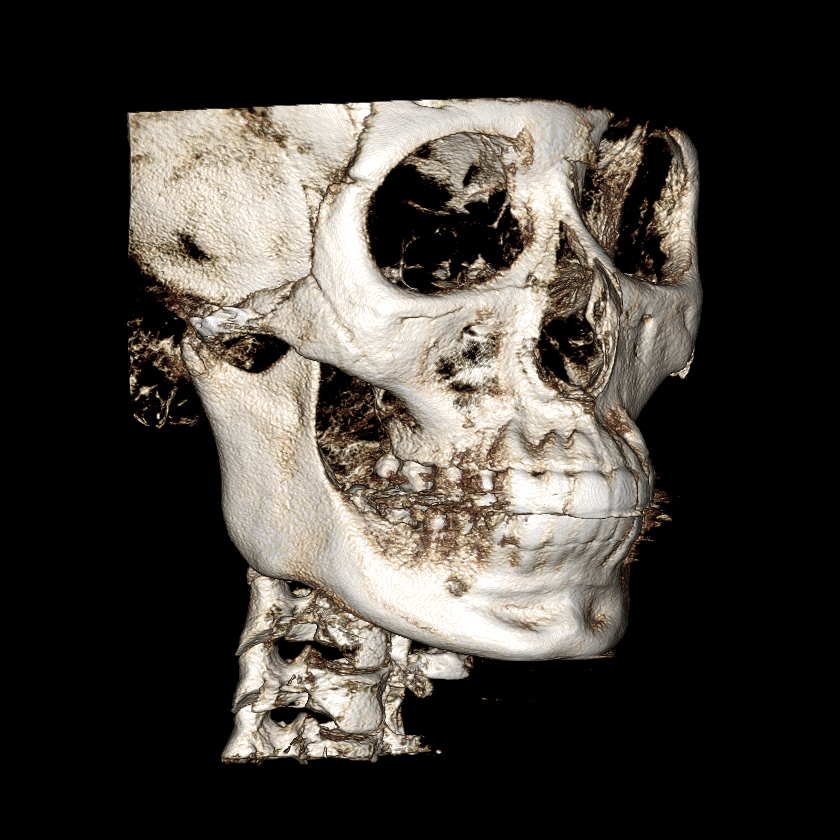
you can see that the bone is actually well united.
However, you should also know that even this image is not expressing the bone with complete accuracy.
To explain this, you need to understand 3D CT.
The facial CT scans we usually take are, in simple terms, multiple X-ray images taken at 5 mm intervals and layered on top of one another.
In fact, 5 mm is a very wide interval.
CT scans taken at university hospitals are done at 1 mm intervals.
However, the downside is that it takes a long time.
In conclusion, CT scans taken at 5 mm intervals to see the overall shape can contain a great deal of distortion.
Also, 3D CT is created graphically through a program based on these axial CT images.
The distortion can become even more pronounced.
Even if a 3D CT makes it look like there is a hole in the bone or that it is separated, when the surgery is actually performed, there are many cases where the bone is completely united.
If you look at the next photo, it may seem as though there is a zygoma gap, but in reality there is no gap at all.

Seeing this, some people worry and conclude that it is zygoma nonunion or a gap.
However, this area has not yet fully undergone calcium deposition, and with time it will be filled in.
Because zygoma gaps and nonunion can look slightly different depending on the viewing angle, it is important to examine the entire CT scan from multiple angles and make an accurate diagnosis.
There are also cases where a zygomatic bone that seemed to be nonunion later rejoins years after surgery, so rather than worrying early at 1 month, 3 months, or even before 1 year after surgery, it seems important to stay a little patient and check the progress with follow-up CT scans after surgery.
For someone being consulted, it may be easier to understand if you think of a bone image that clearly looks separated as true nonunion.
There are also cases where even a slight separation is said to be nonunion and that surgery must be repeated, but if you remember that this kind of distortion exists, it may help when looking at CT scans.
Thank you.