Hello, this is Dr. Jo Hyun-woo of Invertex Plastic Surgery.
Recently, while consulting with patients, I often get questions like, “Are you doing High-L zygoma surgery?”
When I first heard the term, I thought it was just one of the names for zygoma surgery.
But since I hear people talk about it a lot these days, it seems that many doctors explain it as a surgical method.
So today, I’ll explain what High-L zygoma surgery is.
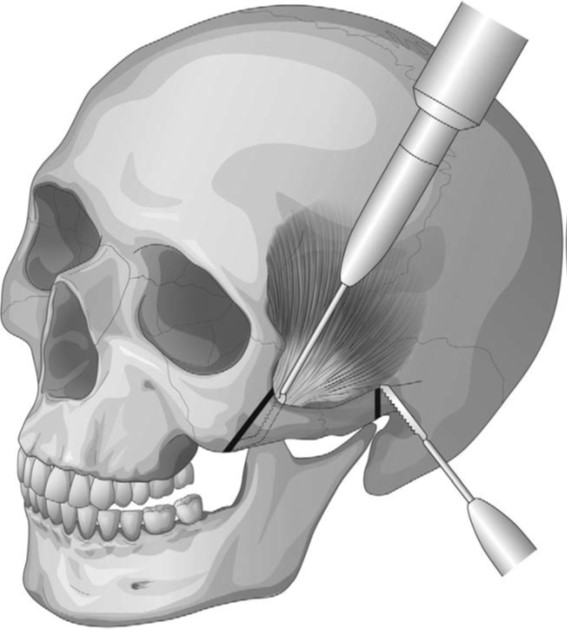
When performing zygoma surgery through an intraoral incision, which is commonly referred to as 3D zygoma surgery, the body of the zygoma is cut in an L-shape.
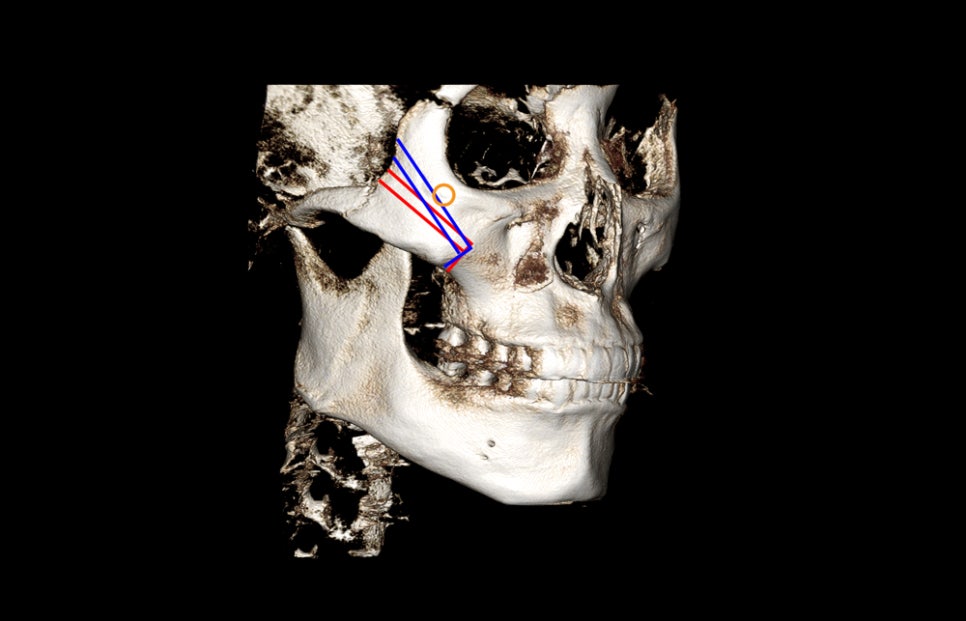
As shown in this diagram, if the red osteotomy line represents the standard zygoma surgery cut line, then the surgery method cut in blue can be considered High-L zygoma surgery. However, even with High-L, the cut cannot always be made as close to the eye socket bone as possible.
Because there is an opening where the nerve, marked in yellow, comes out, the cut is made as high as possible while preserving that nerve.
In some other hospitals, I hear that they may cut close to the eye socket bone regardless of the nerve, but in that case, I cannot know exactly how the nerve is preserved.
Returning to the point,
What are the benefits of cutting the cheekbone as high as possible like this?
First, for patients whose zygoma is wide on the outer side of the eye socket, the effect of narrowing the width of the zygoma can be maximized.
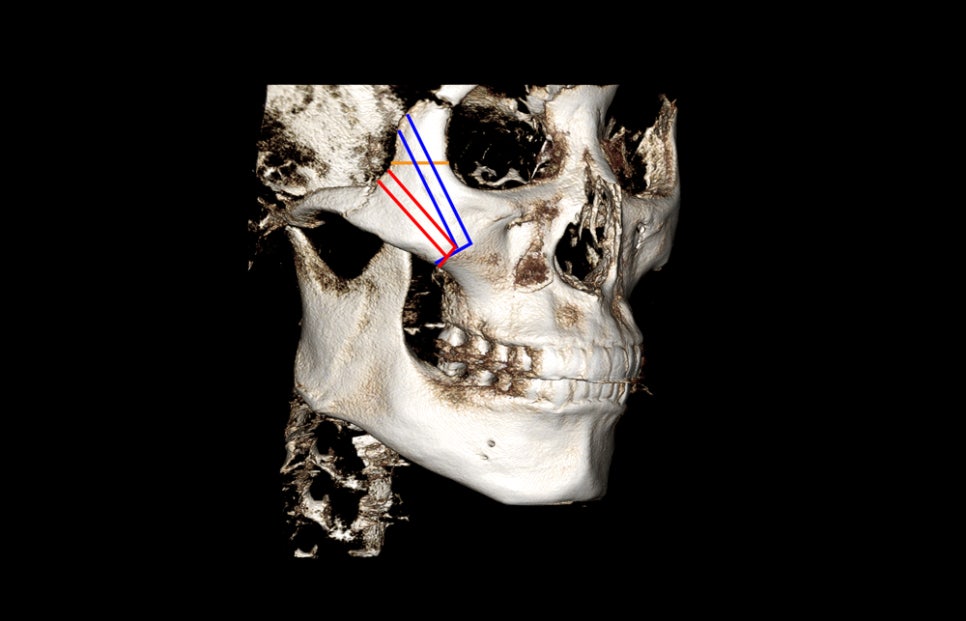
This photo shows a hypothetical osteotomy line that ignores the nerve path.
If the width of the zygoma marked in yellow is wide, then making the cut higher along the blue line reduces the zygoma next to the eye socket significantly, maximizing the effect of zygoma reduction surgery.
However, the shape of the cheekbone varies from person to person, and there are many people whose zygoma is not wide next to the eye socket. In such cases, there is no need to raise the osteotomy line that much.
Another advantage is that it allows an osteotomy that includes the MMP (most maximal high point), which is said to be the highest point of the zygoma, so the reduction of the 45-degree zygoma area can be maximized.
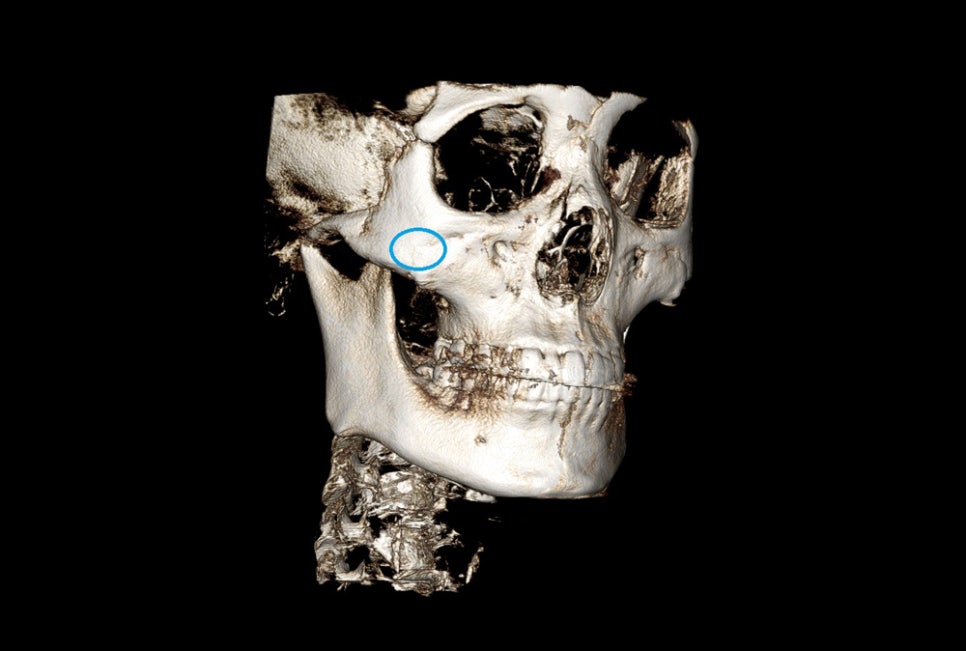
When the osteotomy line is low, the MMP often does not shift much, so there may be cases where patients say they had zygoma surgery but the 45-degree zygoma is still too prominent.

For 3D zygoma surgery, I try to perform it in a High-L style by making the cut right next to the opening where the nerve comes out, as much as possible.
That is because the higher the osteotomy line, the greater the reduction in width can be from the front.
However, cutting off more of the cheekbone is not always better, and if too much of the cheekbone is removed inward, the maxillary sinus may be exposed, so depending on the patient, I try to perform the surgery in the safest direction possible.
At Invertex Plastic Surgery, we perform two types of zygoma surgery: 3D zygoma and 230-degree three-dimensional zygoma.
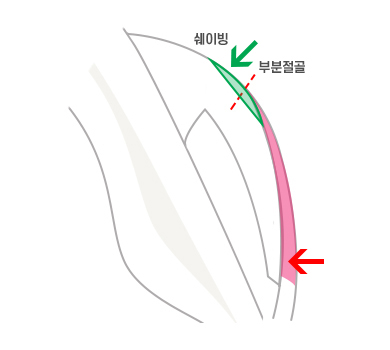
In the case of 230-degree three-dimensional zygoma reduction surgery, the operation is performed using a low osteotomy line.
Because of this, the reduction in the 45-degree zygoma area is insufficient, so the missing part is supplemented by shaving the 45-degree zygoma.
Different surgeons have different thoughts and approaches regarding surgery, but in my case, I believe that performing surgery safely, even if the effect is somewhat reduced, is the best way to minimize side effects that may appear later. So I think it is most important for patients to choose a clinic that performs surgery suited to their own needs.
Today, I briefly talked about High-L zygoma surgery.
It is not a newly introduced surgical method, and most zygoma surgeries are performed in a High-L manner. You can simply think of High-L as a direction in which the osteotomy line is raised a bit higher to increase the effect of the existing zygoma reduction surgery.
I hope this was helpful.
Thank you.