Hello.
I am Dr. Heo Jae-won, a board-certified plastic surgeon at 3D Plastic Surgery, performing youthful facial rejuvenation procedures.
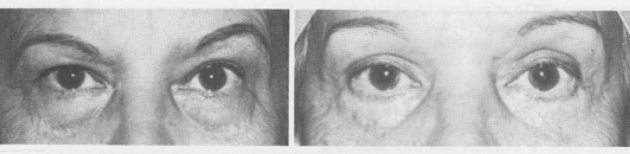
As we age, it is common for the area under the eyes to become puffy, hollow, and covered with more fine lines.
By the time you start hearing that you look tired, or that your expression seems harsher than it actually feels, many people begin searching for a solution and come across “lower blepharoplasty.”
When you actually look into it, even the terminology can be confusing.
There is an abundance of information, but it can be hard to know where to begin.
One reason it has become so complex is that lower blepharoplasty has continued to evolve over time.
Recently, it has also become common to understand this progression by dividing it into generations.

Although it is not an official medical term, it is a very useful way to organize the concepts according to the direction of surgery and changes in technique.
Today, I would like to talk about the first starting point: first-generation lower blepharoplasty.
First-generation lower blepharoplasty: starting from simple 'fat removal'
Early lower blepharoplasty was not as complex or multilayered as it is now.
The core idea was simple: remove the protruding fat to make the under-eye area flatter.
That straightforward goal was first detailed in a 1951 paper by American plastic surgeon Salvadore Castanares.
He explained that the under-eye bulge was caused by weakening of the orbital septum → fat protrusion, and proposed a surgical method that removed the protruding fat through an incision.
The approach that later became the standard was the transcutaneous method.
It involves making an incision in the skin just below the eyelashes, opening the muscle, and removing unnecessary portions from the three fat compartments—medial, central, and lateral.
The advantages of this method were clear.
It could address not only protruding fat but also the remaining skin and wrinkles, and the cosmetic satisfaction was high.
In practice, the surgery was relatively simple, taking about 30 minutes to 1 hour, and many patients were satisfied simply because their under-eye area became flatter immediately after surgery.
However, the drawbacks were also clear: ectropion, hollowing, and loss of aegyo-sal

Over time, the shortcomings of this method became evident.
The most representative complication was ectropion, in which the lower eyelid is pulled downward and the conjunctiva becomes exposed.
In addition, if too much fat was removed, the under-eye area could become hollow, making the face look tired and aged.
We often call this an operated look—an appearance that clearly shows signs of surgery.
If the incision also damaged the orbicularis oculi muscle, which closes the eye, it could lead to loss of the natural aegyo-sal or an awkward facial expression.
What brought attention back as a way to avoid a scar was the transconjunctival approach of the 1980s and 1990s.
Reconsidering the transconjunctival approach: scarless surgery?
In fact, the idea of removing fat without an external incision had already been proposed in 1924 by Bourguet of France.
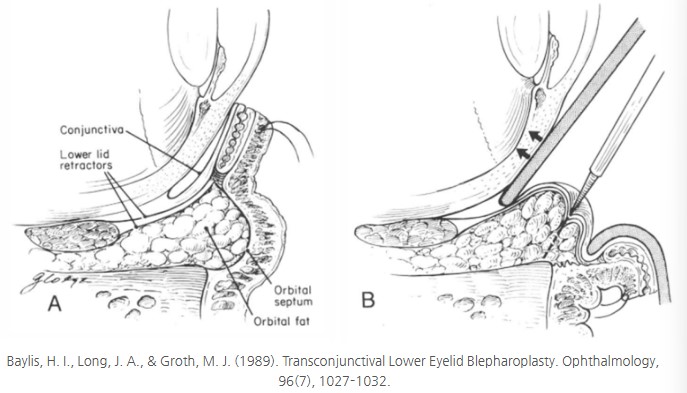
He attempted a non-incisional method, the transconjunctival approach, by accessing the fat through the conjunctiva (the inner lining of the eyelid).
However, at the time, limitations in technique and anatomical knowledge prevented it from becoming widespread.
It was in the 1980s and 1990s that this method came back into the spotlight in earnest.
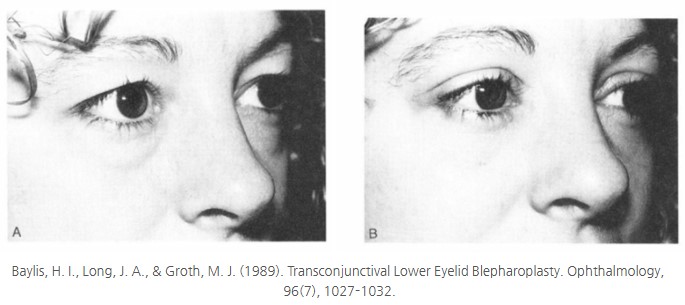
In particular, in 1989, Baylis applied this approach to 122 patients and reported that it produced “no scar, excellent fat removal, and no ectropion.”
This meant that transconjunctival surgery was also cosmetically excellent, especially for younger patients without skin laxity.
However, this method also focused only on removing protruding fat, so it did not address a hollow tear trough or a lack of volume in the midface.
Patients began saying things like, “The bulge under my eyes is smaller, but the tear trough looks deeper,” or “Too much fat was removed, so the under-eye area looks hollow.”
From simple removal → structural understanding: lessons for the next generation
Over time, it became clear that a surgery aimed only at reducing volume could not create a youthful, natural appearance.
Gradually, the idea took hold that fat is not something to simply remove, but an asset that should be repositioned.
In 1981, Loeb first proposed the concept of pulling the fat down toward the tear trough to fill the hollow area,
and in 1995, Hamra developed this more precisely and argued that “fat must be preserved or repositioned.”
This volume-centered approach that emerged in this way became the starting point for second-generation lower blepharoplasty.
In closing: the simpler era, and what we learned from it
First-generation lower blepharoplasty certainly had clear advantages.
It neatly addressed bulging under-eye fat, and the surgery itself was relatively simple.
However, complications such as hollowing, ectropion, and loss of aegyo-sal were not uncommon.
And above all, the fact that the face looked unnatural after surgery ultimately revealed the limitations of this method.
From those trial-and-error experiences, a new paradigm of “preservation” and “repositioning” emerged, and that change led to the next generation.
In the next post, I will go into more detail about second-generation lower blepharoplasty, which began from this reflection—the emergence of fat repositioning techniques and their clinical effects.
Where do your concerns about the under-eye area fit within this progression?
I hope this has been a chance to consider which generation of surgery may be right for you.
If you are interested in a more detailed discussion of lower blepharoplasty, please also visit the link below.
Sincerely,
Dr. Heo Jae-won, Board-Certified Plastic Surgeon